
MOXI Laser Cost 2026: Full Price Guide
Moxi laser cost - Discover the true cost of MOXI laser treatment, from per-session prices to full plans, and learn what drives pricing for real results
Jun 18, 2026

You've cleaned up your diet. You've tried the workouts that used to work. Maybe you've even lost the baby weight, or a significant amount after a major lifestyle change. But the lower belly still pushes forward, especially when you sit up in bed, lift a laundry basket, or try a plank.
That experience is frustrating because it often gets mislabeled as “just loose skin,” “stubborn fat,” or a lack of effort. In many people, the issue is diastasis recti, a separation in the connective tissue between the abdominal muscles. It's common after pregnancy, and it can also show up after major weight changes. Beyond how your abdomen looks, it can affect how your core functions.
I talk to many patients who feel confused by mixed advice. One person is told to do more ab exercises. Another is told surgery is the only answer. Most need something much more practical: a clear way to decide whether symptoms can improve with therapy, when repair makes sense for function, and which type of repair actually fits their body and goals.
A common story goes like this. A mother is several months, sometimes several years, past delivery. She's back to walking, eating well, and trying to strengthen her midsection. But every time she engages her core, she sees a ridge or a soft bulge down the center of her abdomen. Her back feels tired. Her core feels unreliable. Clothes fit differently even though the scale has changed.
Another version happens after weight loss. Someone has done the hard work of changing their health, but the abdomen still feels weak and unsupported. They can't tell whether they're dealing with extra skin, residual fat, a hernia, or something else.
Often, that “something else” is diastasis recti. This isn't a character flaw, and it isn't laziness. It's a structural issue in the abdominal wall. The tissue that normally holds the two sides of the rectus muscles together becomes stretched and thinned, so the midline loses tension.
Many patients feel relief simply learning that the bulge has a name and that it can be evaluated like any other medical problem.
That matters because the next step depends on what the bulge represents. If the issue is primarily skin laxity, the solution looks different than if the issue is a weakened abdominal wall. If the main problem is function, such as poor core support, discomfort, or instability, then the conversation becomes less about appearance and more about reconstruction.
Some people improve with focused physical therapy. Others continue to struggle despite doing all the “right” things. Those are the patients who often ask the most important question: not “Can this be fixed?” but “What kind of fix makes sense for me?”
Think of the front of your abdomen like a jacket with a zipper running down the middle. The two sides of the jacket are your rectus abdominis muscles. The zipper is the linea alba, the connective tissue that joins them in the center. In diastasis recti, that zipper doesn't exactly break, but it stretches and thins. The two muscle columns drift apart, and the center of the abdomen loses firmness.
That's why this condition can look like a round, persistent bulge. It's not always fat. It's often a loss of tension in the abdominal wall itself.
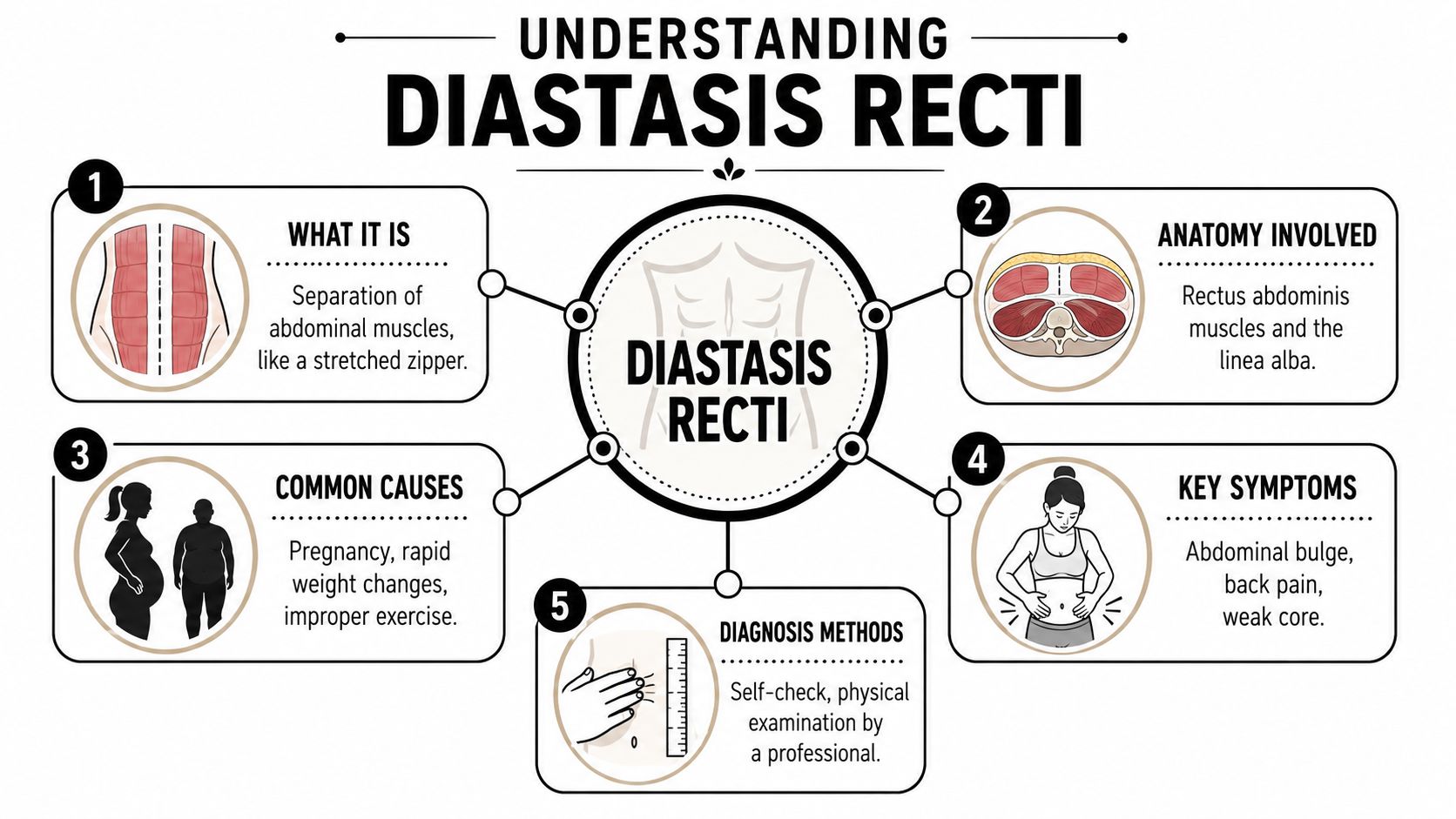
Pregnancy is the classic cause because the abdominal wall has to expand to accommodate a growing uterus. Major weight fluctuations can create similar strain. Some exercise patterns can also worsen pressure through the midline, especially when the deep core isn't controlling the movement well.
One reason the condition matters so much is that it can persist long after the postpartum period. A 2024 longitudinal study in Scientific Reports found that using an inter-rectus distance of more than 2 cm as the diagnostic threshold, prevalence was 36% at 3 years, 31% at 5 years, and 30% at 30 years postpartum.
Some people notice appearance first. Others notice function first.
Common clues include:
A home check can be helpful, though it doesn't replace an exam.
This can tell you that something may be going on, but it can't tell you the full story. A clinician needs to determine whether the issue is mild tissue laxity, a more significant separation, or a hernia that needs a different plan.
Practical rule: A bulge is a symptom, not a diagnosis. The treatment depends on what's causing the bulge.
Many people assume any core exercise will help. That's one of the biggest mistakes I see. With diastasis recti, some exercises support healing and control. Others increase pressure and make the separation more obvious.

Targeted physiotherapy is first-line treatment, particularly after pregnancy. The key is training the deep core, especially the transversus abdominis, rather than repeatedly forcing the outer abdominal wall forward. The Cleveland Clinic's guidance on diastasis recti notes that surgical referral is indicated only after patients with significant functional impairment have failed a minimum 6-month core-training physiotherapy program. The same guidance also states that crunches and planks can worsen the condition.
The best therapy plans usually look gentle from the outside, but they're highly specific.
Useful elements often include:
If you're trying to understand how movement specialists coordinate different approaches to spine, posture, and body mechanics, this guide comparing physical therapy and chiropractic care can help clarify the difference.
A lot of popular ab work is poorly suited to this condition, especially early on.
Avoid movements that create a visible “cone” or “dome” down the center of the abdomen, such as:
A video demonstration can make these movement ideas easier to picture:
Physical therapy can improve control, reduce symptoms, and help some patients narrow the separation. It may also help you determine whether the main problem is weak muscle coordination or a structural loss of tension that exercise can't fully reverse.
For patients whose concern is mostly mild skin laxity rather than a true abdominal wall problem, non-surgical options may also be part of the discussion. Some people explore treatments for skin quality, such as non-invasive skin tightening, though that's a different issue from repairing the abdominal wall itself.
The question isn't merely whether surgery can close the gap. The better question is whether diastasis recti repair is needed to restore function after appropriate therapy hasn't done enough.
That distinction matters. Surgery shouldn't be the first move for most patients. But it also shouldn't be dismissed as “just cosmetic” when the abdominal wall is failing to do its job.
People often describe the same pattern in different words. “My core feels disconnected.” “My back gets tired quickly.” “I can't generate support when I lift.” “I still look pregnant by evening.” These complaints may sound cosmetic on the surface, but they often reflect poor force transfer through the trunk.
When symptoms persist after dedicated rehabilitation, surgery becomes a reconstructive conversation.
High-quality evidence summarized in a review on treatment options for diastasis recti shows that surgical reconstruction can improve core stability, back muscle strength, quality of life, and urinary incontinence in symptomatic patients who did not improve with at least 6 months of core training.
Surgery is worth discussing when several of these are true:
Surgery can be the right choice when the abdomen isn't simply loose. It's mechanically underperforming.
A related source of confusion is terminology. Some patients hear “tummy tuck” and assume that means the operation is purely aesthetic. In reality, many abdominal contouring procedures include muscle repair because the anatomy and the symptoms overlap. If you want a clearer breakdown of that procedure, this overview of what a tummy tuck procedure involves is a useful starting point.
There isn't one standard operation for everyone with diastasis recti. The right method depends on your anatomy and on what you're trying to fix. Some patients need only internal repair of the abdominal wall. Others need that repair plus removal of extra skin. That's why the same diagnosis can lead to very different surgical plans.
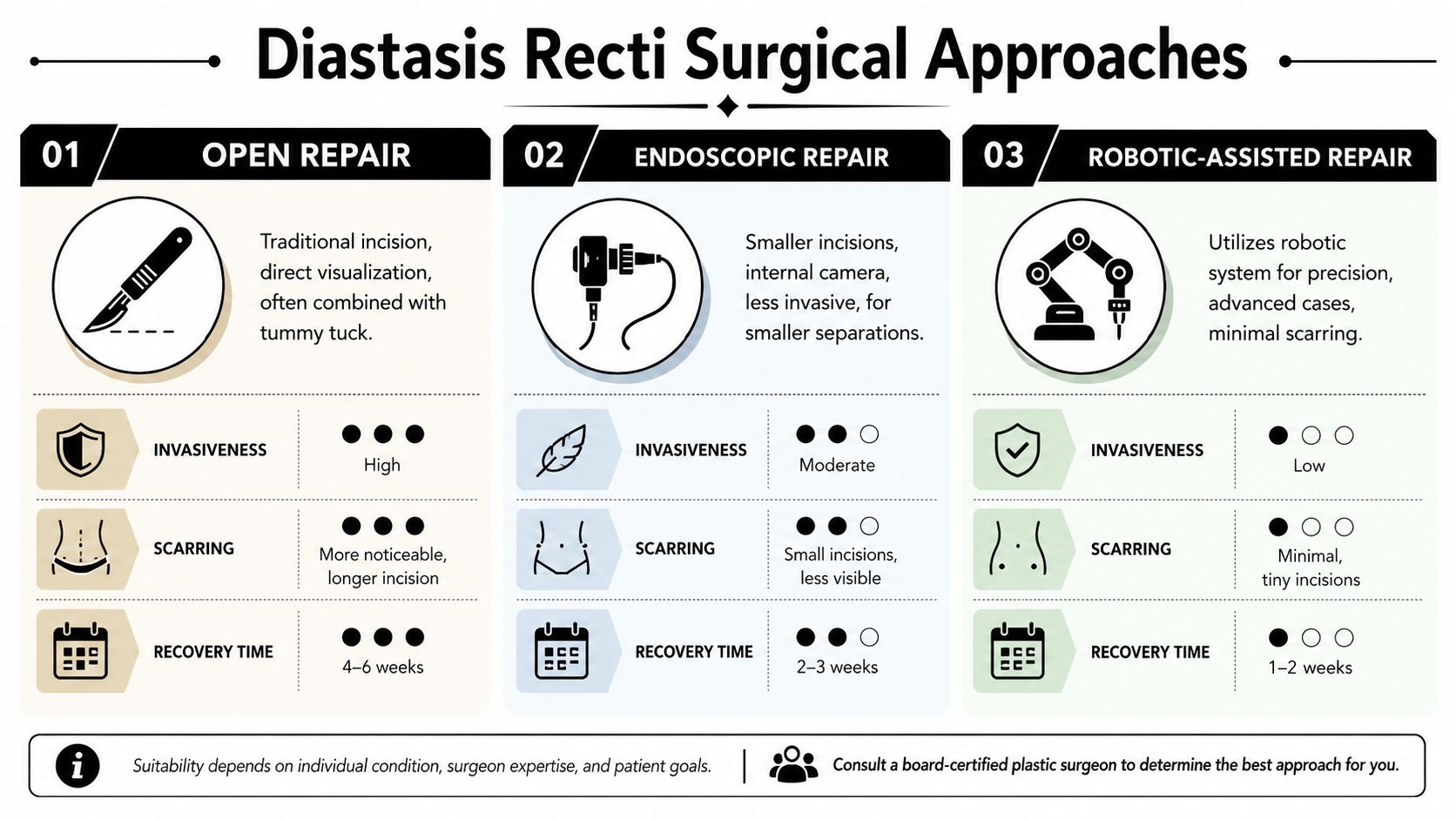
This is the approach many patients know best. When excess skin and soft tissue are part of the problem, an open repair allows the surgeon to tighten the abdominal wall and address the overlying contour in the same procedure.
In plain language, this is often the best match when you're saying, “My muscles feel separated, but I also have loose skin that no exercise will remove.”
Typical strengths of open repair:
Some patients have a true diastasis but very little excess skin. In those cases, laparoscopic or other minimally invasive approaches may be considered. The appeal is straightforward: smaller incisions and no full tummy tuck when skin removal isn't necessary.
This approach may fit the patient who says, “I don't mind my skin. I mind the weak, protruding core.”
A few tradeoffs matter:
| Approach | Best suited for | Main advantage | Main limitation |
|---|---|---|---|
| Open repair | Patients with muscle separation plus loose skin | Can combine wall repair and contouring | Larger scar pattern |
| Minimally invasive repair | Patients with separation but limited extra skin | Smaller incisions | Doesn't remove significant loose skin |
| Robotic-assisted repair | Selected patients in experienced hands | Precision and minimally invasive access | Strong outcome data remain limited |
Some repairs use sutures alone. Others add mesh reinforcement, especially when added support is desirable. Patients sometimes worry that mesh automatically means something has gone wrong or that it's only used for hernias. That isn't the case. In abdominal wall reconstruction, mesh can function like an internal support layer.
Technique matters. An overview of management published in the Global Journal of Surgery and Case Reports cites a systematic review showing recurrence in 6% of suture-only repairs versus 0.6% in repairs using mesh. The same review notes that modern practice commonly combines rectus fascia plication with retro-rectus mesh onlay, and polypropylene is the most frequently used mesh material in reported repairs.
The best operation isn't the newest or the smallest. It's the one that solves the actual problem you have.
A useful way to think about it is to separate your goals into three buckets:
Those goals don't compete, but one of them usually leads. That lead goal often determines which surgical strategy makes the most sense.
Recovery after diastasis recti repair is easier when you understand what your body is trying to do. The repair needs time to hold. Swelling needs time to settle. Your muscles need time to work in their new position without being overstrained too early.
Many individuals feel better when recovery is broken into phases rather than treated as one long, vague waiting period.
The first part of recovery is about protection and gentle movement. You'll usually be walking in a bent or guarded way at first, especially if skin was removed as part of the procedure. That's normal. Patients often describe tightness more than sharp pain.
Your surgeon may recommend:
As the initial soreness fades, people can become overconfident. That's when setbacks happen. Feeling better doesn't mean the repair is ready for full exercise, twisting, heavy lifting, or aggressive ab training.
Ask your surgeon specific questions about:
Healing is not just about what you can tolerate. It's about what the repair can safely withstand.
For postpartum patients who are still juggling nursing pillows, abdominal support, hydration, and practical comfort items at home, a thoughtfully organized postpartum recovery toolkit for new moms can make the home side of recovery easier to manage.
Every operation has risks, and your own surgeon should review them in detail based on your health and the exact procedure planned. In general, concerns after abdominal surgery can include healing problems, contour irregularity, fluid collection, discomfort, numbness, and recurrence. The specific risk profile can differ between a limited internal repair and a more extensive operation that includes skin removal.
Call your surgeon promptly if something feels off, especially increasing swelling on one side, worsening redness, drainage, fever, or pain that's escalating rather than gradually improving.
Patients often expect a flat, final-looking abdomen right away. In reality, the abdomen can stay swollen, tight, and uneven for a while. Early improvement is often visible, but the more settled result takes patience.
What you're usually watching for over time is this: less bulging with strain, better support through the middle, and a more natural relationship between posture, movement, and the abdominal contour you see in the mirror.
A consultation is where a broad topic becomes personal. Two people can both have diastasis recti and need very different recommendations. One may benefit from internal repair only. Another may need a more extensive operation because skin excess is a major part of the picture.
That's why individualized planning matters so much.
During a thoughtful consultation, the surgeon examines the abdominal wall, evaluates skin quality and contour, and listens closely to what bothers you most. Sometimes the answer is straightforward. Sometimes the key issue is teasing apart whether the main problem is muscle separation, loose skin, a hernia concern, or some combination.
A visit should also leave you with practical clarity. You should understand what surgery can improve, what it won't change, what scar pattern to expect, and whether your goals point toward an open or minimally invasive approach.
Authoritative reviews discussed by the American Society of Plastic Surgeons note that while multiple techniques exist, including open and minimally invasive approaches, the best method depends on the patient's goals regarding skin removal, scarring, and recovery time.
Patients usually get more from a consultation when they arrive with a symptom list and clear priorities. Write down what you feel during daily activities, what you've already tried, and what outcome matters most to you.
If you'd like a practical guide before that appointment, this article on what happens at an initial plastic surgery consultation and how to prepare can help you organize your questions and expectations.
Coverage varies, and the answer often depends on how the procedure is documented and why it's being done. When the surgery is framed only as cosmetic contouring, coverage is less likely. When there are clear functional symptoms and supporting examination findings, the conversation may be different.
Policies differ widely, so the safest approach is to ask your surgeon's office what documentation may be needed and then verify details directly with your insurer before scheduling surgery.
Yes, but the scar pattern depends on the operation. An open repair combined with skin removal creates a more noticeable scar than a minimally invasive repair performed through smaller incisions. That tradeoff is often worth it when loose skin is a major part of the problem.
The more useful question isn't “Will there be a scar?” It's “Does this scar buy me the correction I need?” In many patients, that's the right way to think about it.
Future pregnancy can place the abdominal wall under the same kinds of stress that caused the separation in the first place. For that reason, many surgeons prefer to time repair after childbearing is complete when possible.
That doesn't mean every future pregnancy ruins a repair, but it does mean pregnancy can stretch the tissues again and affect both function and contour. If more children are possible, discuss that early. Timing matters.
No. That's one of the biggest misconceptions around this condition. Some patients do seek improvement mainly for contour, but others are pursuing surgery because the abdominal wall no longer feels mechanically sound.
When a patient has done appropriate therapy and still has persistent symptoms such as poor core support, back discomfort, or functional limitation, diastasis recti repair can be part of restoring abdominal wall integrity rather than solely changing shape.
If you're dealing with a persistent abdominal bulge, core weakness, or symptoms that haven't improved with focused therapy, Cape Cod Plastic Surgery offers expert evaluation and personalized treatment planning. A consultation can help you understand whether your concern is skin laxity, muscle separation, or a combination of both, and what type of repair best fits your goals.
Moxi laser cost - Discover the true cost of MOXI laser treatment, from per-session prices to full plans, and learn what drives pricing for real results

August 1, 2026
Achieving a Refreshed Appearance Through Advanced Eyelid Rejuvenation

August 1, 2026
Preparing for Your Plastic Surgery Consultation: A Document Checklist
Cape Cod Plastic Surgery offers expert cosmetic and reconstructive procedures in a safe, accredited setting. Led by Dr. Marc Fater, we combine advanced techniques with personalized care to help you look and feel your best.
Monday: 9:00 AM – 5:00 PM
Tuesday: 9:00 AM – 5:00 PM
Wednesday: 9:00 AM – 5:00 PM
Thursday: 9:00 AM – 5:00 PM
Friday: 9:00 AM – 5:00 PM