
How to Get Rid of Wrinkles Between Eyebrows: Surgeon's Guide
Tired of frown lines? Learn how to get rid of wrinkles between eyebrows with at-home tips, Botox, fillers, and more from a board-certified plastic surgeon.
May 21, 2026

Wanting fuller breasts without committing to a lift is a common place to start. Most patients I meet aren't asking for a dramatic change. They usually want restored volume, better upper-pole fullness, and a shape that looks more balanced in clothing and without it. At the same time, they're often hesitant about the extra scars and recovery that come with mastopexy.
That's a reasonable concern. Breast augmentation without lift can be an excellent option, but only when the anatomy supports it. The decision isn't based on preference alone. It depends on nipple position, skin elasticity, breast tissue quality, and how much sagging is already present.
A good consultation should answer one central question clearly: will implants alone improve your shape, or will they only make a low breast larger? That distinction matters. Volume and lift are not the same thing, and when they're confused, patients end up disappointed.
Many people considering surgery are trying to solve two problems at once. They want more fullness, but they also want a breast shape that sits better on the chest. The catch is that those goals don't always come from the same operation.
If your breasts have lost volume after pregnancy, weight change, or aging, implants may restore that fullness very well. If the breast position is still reasonably good and the nipples sit high enough, augmentation alone can create a rounder, more lifted-looking result. In the right patient, that can mean a meaningful improvement with fewer incisions than a lift would require.
If the nipple has descended or the lower breast skin has stretched significantly, implants don't correct that anatomy. They fill. They don't tailor.
Practical rule: The best result comes from matching the operation to the problem. Volume loss responds to augmentation. Excess skin and low nipple position respond to lift surgery.
That's why this decision has to be made carefully. A surgeon should assess not only what you want to look like, but also what your tissue can support over time. A result that looks acceptable in the early weeks can drift if the skin is lax and the implant is doing work that should have been done by a lift.
A thoughtful plan starts with honest anatomy, not wishful thinking.
Breast augmentation without lift works best when the breast already has a decent framework and needs more volume. A straightforward way to think about it is this: adding an implant is like refilling a slightly deflated shape. A lift is more like reshaping the envelope itself.

An implant can:
That distinction between augmentation and lift shows up clearly in procedure trends. In 2022, about 143,364 breast lift procedures were performed in the U.S., while almost 300,000 breast augmentations were done, showing that augmentation remains roughly twice as common in a major cosmetic market. The same guidance also notes that, unlike an implant, a breast lift does not predictably restore volume to the upper portion of the breast (clinical overview of augmentation versus lift goals).
For readers comparing procedures side by side, this discussion of when and why to consider breast lift surgery helps frame the difference in goals.
Implants don't:
That's where disappointment usually starts. If the nipple is already too low, putting a larger implant underneath it may create a fuller breast, but not a better-positioned one. In some patients, it can make the bottom of the breast look heavier.
Filling a breast is not the same as lifting a breast.
The right candidate often sees a pleasing shape change from implants alone. The wrong candidate gets more size without enough improvement in position.
This is the section patients should pay the closest attention to. Candidacy for breast augmentation without lift is mainly an anatomical decision. It depends less on what you hope implants will do, and more on what your breast tissue will allow them to do.
A key checkpoint is nipple position relative to the inframammary fold, which is the crease under the breast. Expert discussions note that augmentation alone can create a fuller, slightly lifted appearance when nipples sit above the breast fold and skin elasticity is good. The same discussions make clear that significant ptosis is a poor fit for implants alone because the implant does not reposition the nipple or remove excess skin (anatomy-based discussion of augmentation candidacy).
Here is the basic visual framework:

Surgeons often describe breast sagging as ptosis. In practical terms, ptosis grading asks where the nipple sits compared with the breast crease and how much breast tissue hangs below it.
| Ptosis Grade | Nipple Position | Suitable for Augmentation Alone? |
|---|---|---|
| Grade I | Nipple at or just below the inframammary fold | Often yes, depending on skin quality and tissue support |
| Grade II | Nipple below the fold but still above the lowest breast contour | Sometimes borderline, often needs careful planning |
| Grade III | Nipple clearly below the fold and at the lower breast contour | Usually no |
| Pseudoptosis | Nipple above the fold, but lower breast tissue hangs below it | Sometimes, especially if skin quality is still good |
Grade I and some pseudoptosis cases are where augmentation alone can work nicely. Grade II is the gray zone. Grade III usually needs a lift if the goal is a breast that sits higher and looks properly reshaped.
Two patients can have similar nipple position and very different outcomes because their skin behaves differently. Elastic skin supports an implant. Lax skin stretches around it.
I pay close attention to:
A patient with mild droop and firm skin may do beautifully with implants alone. Another with the same apparent droop but poor skin tone may look better with a lift or a staged plan.
Here's a useful video overview before you book a consultation:
You can ask yourself a few practical questions:
Borderline anatomy is where surgical judgment matters most. That's also where an in-person exam matters more than photos.
A patient with mild droop, decent skin recoil, and nipples still sitting in a favorable position may have several reasonable surgical paths. The right plan is not just about choosing an implant. It is about matching implant size, shape, and placement to how the breast tissues behave today, and how they are likely to age over time.
At Cape Cod Plastic Surgery, I plan augmentation without a lift by looking at what the tissues can support. That often means choosing a more conservative implant than a patient expected, especially in borderline anatomy where too much weight can make droop more obvious rather than less.
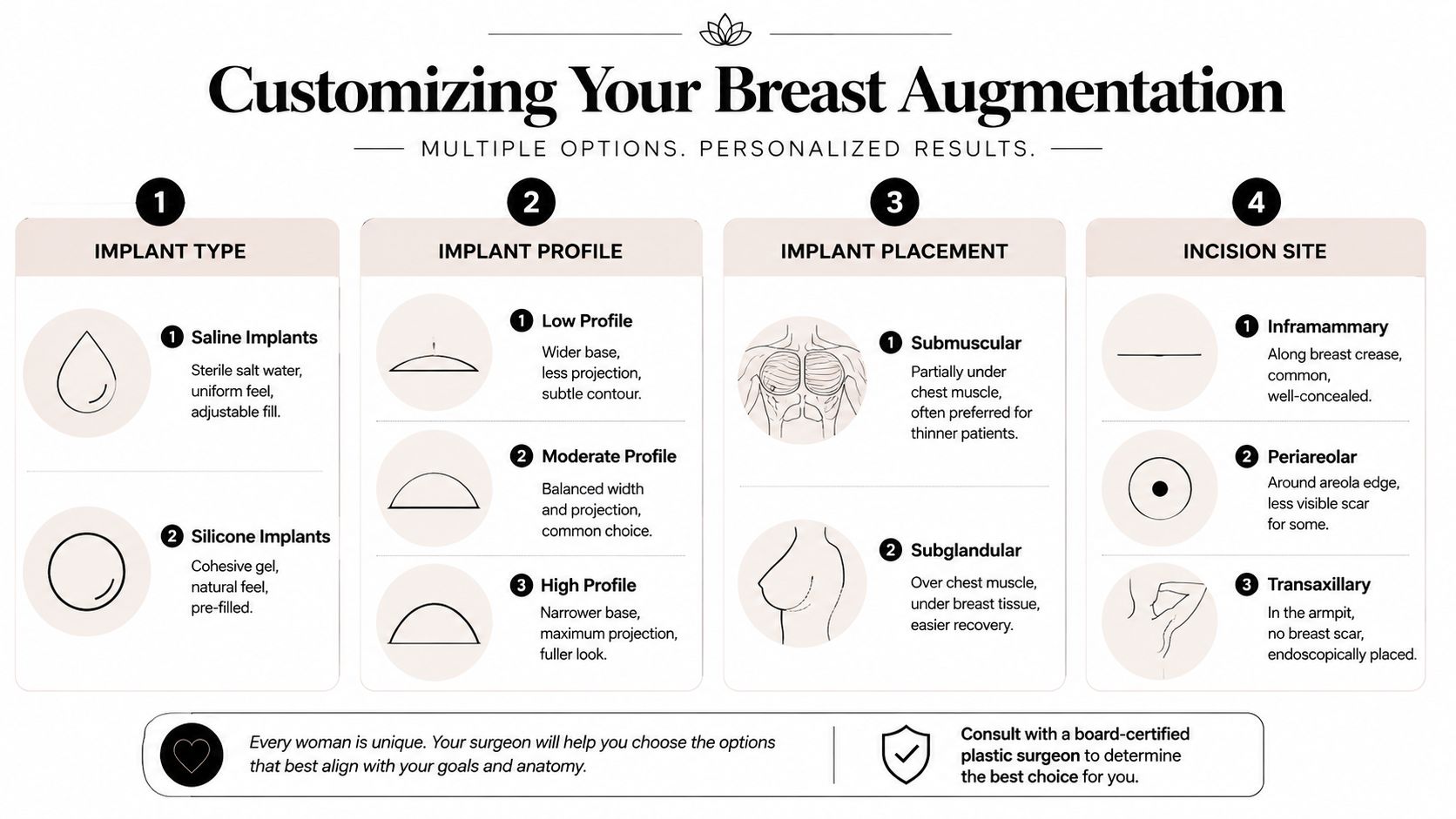
Most patients are deciding between saline and silicone implants. Both can work well. The better choice depends on tissue thickness, desired feel, incision plan, and how much upper-pole fullness the breast can carry without looking overstretched.
Profile matters just as much as fill. A high-profile implant gives more forward projection on a narrower base. A moderate-profile implant spreads volume over a wider footprint. In a breast with borderline ptosis, the wrong profile can make the lower pole look heavier or leave the upper breast flatter than expected.
Patients who want a closer look at material differences can read this comparison of saline and silicone breast implants.
Pocket choice changes both appearance and support. In a no-lift augmentation, I commonly consider three approaches:
Subglandular placement
The implant sits over the muscle and under the breast tissue. This can work in patients with enough tissue coverage and good skin tone.
Submuscular placement
The implant sits at least partly beneath the chest muscle. This often improves implant coverage in thinner patients.
Dual-plane placement
The upper part of the implant is covered by muscle, while the lower breast is allowed to drape more naturally over it. In selected mild cases, that can improve shape and give limited nipple elevation without adding lift scars.
The American Society of Plastic Surgeons discusses dual-plane augmentation as one option in patients deciding between implants alone and a lift, particularly when the anatomy is borderline (ASPS discussion of implant position and lift alternatives).
Dual-plane surgery has limits. It can help with mild glandular descent. It does not correct true nipple malposition or significant skin excess. In those cases, forcing augmentation alone usually leads to a breast that is fuller, but still low.
The most common incisions are inframammary, placed in the breast crease, and periareolar, placed along the areola border in selected patients. Each option has trade-offs in scar location, visibility, surgical exposure, and control of implant position.
For many patients, the more important decision is whether to do everything at once. If the breast sits in a gray zone between augmentation alone and augmentation with mastopexy, a staged plan can be reasonable. That may mean placing an implant now, allowing the tissues to settle, and deciding later whether the shape is good enough or whether a lift would improve the result.
I discuss that option most often with patients who want more volume now but are hesitant about lift scars, or with patients whose skin quality makes the final shape hard to predict in one operation. A staged approach involves two procedures and two recoveries, but it can make the trade-offs clearer and sometimes leads to better long-term decision-making.
For patients seeking a small increase in volume or minor contour refinement, fat grafting may also enter the discussion. It does not replace implants when the goal is a more noticeable size change, but it can be useful in selected cases.
Not being a good candidate for augmentation alone doesn't mean you're out of options. It usually means the surgical plan has to match the anatomy more accurately.

If a patient has lost both volume and position, augmentation-mastopexy often addresses the underlying problem. The implant restores fullness. The lift reshapes the skin envelope and repositions the nipple.
That growing focus on sag correction is reflected in long-term procedure trends. According to the American Society of Plastic Surgeons, 290,224 breast augmentation procedures were performed in 2013, a 37% increase since 2000, while breast lifts increased from fewer than 53,000 in 2000 to 90,006 in 2013, a 70% increase. ASPS also reported nearly 300,000 breast augmentation procedures in 2022 (ASPS statistics on breast lift growth versus implants). The larger point is that while augmentation remains extremely common, lift surgery has grown faster because patients and surgeons increasingly recognize that sag and volume are separate issues.
Some patients are borderline candidates or strongly prefer to avoid a lift now. In that setting, a staged approach can be reasonable: implants first, then a lift later if pregnancy, weight change, aging, or tissue stretch changes the result.
This can make sense when:
The right question isn't only “Can I avoid a lift now?” It's also “What plan gives me the most predictable shape over time?”
Patients usually run into trouble when they try to substitute implant size for a lift. A larger implant can temporarily fill stretched skin, but it can also place more stress on that skin. Over time, that can accentuate lower-pole fullness in a way that doesn't look youthful or balanced.
A long-term plan should include the possibility that breasts will continue to change. Surgery doesn't stop aging, pregnancy-related changes, or shifts in body weight. Good planning respects that from the start.
Recovery after breast augmentation without lift is usually more straightforward than recovery from a combined augmentation-mastopexy, but it still unfolds in phases. Patients do better when they expect a progression rather than an instant final result.
The first 48 hours are usually the most restrictive. The chest feels tight, the breasts sit high, and swelling can make the shape look firmer and less natural than it will later. Most patients are up and walking, but they're taking it easy and avoiding lifting, reaching, and strenuous activity.
A support bra, good hydration, and careful adherence to post-op instructions matter here. Rest helps, but so does light movement.
During the first week, soreness usually becomes more manageable. Follow-up visits are important because they let your surgeon monitor implant position, incision healing, and early symmetry.
By the following weeks, many patients return to routine non-strenuous activity, though exercise restrictions usually continue for a period of time. This is also when people start asking whether they'll need another procedure someday. That question is fair. Educational guidance on staged planning notes that augmentation and mastopexy solve different problems, and that a staged approach may be appropriate when ptosis is substantial (overview of why some patients later need a lift).
For a more detailed week-by-week overview, this breast augmentation recovery timeline is a useful reference.
Over the next several months, implants soften and settle. Swelling decreases. The lower pole rounds out, and the final shape becomes easier to judge.
That's also when the value of correct preoperative planning becomes obvious. If the breasts were a good match for augmentation alone, the result tends to look fuller and more balanced as healing progresses. If the tissues were too lax from the start, that limitation often becomes more visible as the early swelling fades.
A good consultation should leave you with more clarity, not more confusion. Bring questions. The best discussions are specific.
A consultation is most productive when you ask not only what can be done, but also what should not be done.
They can if the breast skin is already lax and the implant is doing work that should have been done by a lift. That's one reason oversized implants in borderline anatomy often age poorly.
Yes. Mild sagging can improve visually when the nipple remains high enough and the skin still has good elasticity. The key is whether the implant is restoring fullness or trying to substitute for a lift.
Not always. In some patients, it's the more controlled plan. It allows volume to be restored first and reserves lifting for a later point if tissue changes make it necessary.
Look at your bra fit and side profile. If the issue is emptiness at the top with otherwise reasonable position, that points more toward augmentation. If the nipple sits low or points downward, shape correction usually becomes a larger part of the discussion.
The next step is a personal exam and a direct conversation about your anatomy, goals, and long-term plan. If you're considering Cape Cod Plastic Surgery, schedule a consultation with Dr. Marc Fater to find out whether breast augmentation without lift is a good match for your tissue, or whether a lift or staged approach would give you a more reliable result.
Tired of frown lines? Learn how to get rid of wrinkles between eyebrows with at-home tips, Botox, fillers, and more from a board-certified plastic surgeon.

July 4, 2026
Planning a brow lift in Cape Cod? Understand your brow lift recovery time with our patient guide on what to expect, aftercare, and healing milestones.

July 3, 2026
Explore the 2026 breast implants price range, from national averages to local Cape Cod costs. Learn what's included and how to get an accurate quote.
Cape Cod Plastic Surgery offers expert cosmetic and reconstructive procedures in a safe, accredited setting. Led by Dr. Marc Fater, we combine advanced techniques with personalized care to help you look and feel your best.
Monday: 9:00 AM – 5:00 PM
Tuesday: 9:00 AM – 5:00 PM
Wednesday: 9:00 AM – 5:00 PM
Thursday: 9:00 AM – 5:00 PM
Friday: 9:00 AM – 5:00 PM