
Skin Tightening After Liposuction: Options & Recovery
Considering skin tightening after liposuction? Explore recovery, influencing factors, and effective treatment options, from non-invasive to surgical.
Apr 14, 2026
You may be reading this after doing something very hard. You lost a significant amount of weight. You improved your health. People may even tell you that you should feel “done.”
But you’re not done if a heavy fold of lower abdominal skin still causes rashes, pulls on your back, gets in the way of exercise, or makes daily hygiene frustrating. That’s where many patients start asking a practical question: what is a panniculectomy procedure, and could it help me feel functional again?
A panniculectomy isn’t about chasing a perfect stomach. It’s a reconstructive operation designed to remove the overhanging apron of excess skin and fat, called a pannus. For many patients, that tissue remains after major weight loss, including after bariatric surgery. If you’re in that position, learning more about body contouring after weight loss can help you see where a panniculectomy fits in the larger recovery journey.
The simplest way to understand a panniculectomy is this. It removes the hanging tissue in the lower abdomen when that tissue is causing real problems.
Those problems often sound very ordinary, which is why they’re easy to dismiss. Skin irritation. Moisture trapped in the fold. Trouble keeping the area clean. Clothing that rubs. A sense of heaviness when you walk or stand for long periods. Yet those “ordinary” issues can affect comfort every single day.
A panniculectomy removes excess abdominal skin and fat known as a pannus. Its primary purpose is functional improvement, not cosmetic reshaping. It’s commonly performed after massive weight loss, including after bariatric surgery, according to a large review of patients undergoing abdominal panniculectomy published by the National Library of Medicine and PubMed Central: https://pmc.ncbi.nlm.nih.gov/articles/PMC8613336/
That distinction matters. A lot of patients assume this is just another name for a tummy tuck. It isn’t. A panniculectomy focuses on removing burdensome tissue. It does not center on muscle tightening or creating a more sculpted waist.
A good way to think about it is this. A panniculectomy aims to make life easier to live in your body, not simply different to look at.
After substantial weight loss, the skin doesn’t always shrink back. When the lower abdominal skin hangs low enough, it can interfere with movement, hygiene, and skin health.
For some people, the next step after weight loss isn’t more dieting or more exercise. It’s removing tissue that won’t respond to either.
That’s why this operation often feels less like an elective beauty treatment and more like the final stage of rebuilding function.
Candidacy starts with one basic issue. Is the lower abdominal overhang causing symptoms, or are you mostly hoping for a flatter, more cosmetic look?
If your main concern is rash, hygiene, discomfort, or physical interference from the hanging tissue, a panniculectomy may be the right category of surgery. If your goal is a tighter abdomen with muscle repair and more aesthetic shaping, that usually points in a different direction.

Panniculectomy is commonly performed after major weight loss. A study found that patients undergoing the procedure had a mean age of 51.7 years, a mean BMI of 33 kg/m² at the time of surgery, and had lost an average of 116 pounds before surgery: https://pmc.ncbi.nlm.nih.gov/articles/PMC8613336/
That doesn’t mean you need to match those numbers. It does show the typical pattern. Many patients have worked hard to lose weight and are left with a persistent abdominal apron that lifestyle changes can’t remove.
Surgeons often describe the size of the pannus on a grade 1 to 5 scale, with lower grades hanging less far and higher grades extending much farther down the body. The grading system helps guide medical necessity and surgical planning, according to the American Society of Plastic Surgeons quality resource on abdominoplasty and panniculectomy: https://www.plasticsurgery.org/documents/medical-professionals/quality-resources/Measure-Specifications-Abdominoplasty-Panniculectomy.pdf
Here’s the practical meaning:
You don’t need to self-diagnose your grade perfectly. What matters is whether the tissue is hanging enough to create skin problems, mobility limitations, or hygiene challenges.
A surgeon also looks at your overall readiness for surgery.
That often includes:
Practical rule: The best candidates aren’t just bothered by the pannus. They’re medically optimized enough to heal safely.
Some patients clearly need in-person evaluation before making assumptions:
A consultation helps separate what’s functional from what’s cosmetic. That distinction drives both the surgical plan and the insurance conversation.
This is one of the biggest points of confusion. Patients often use the terms interchangeably, but they are not the same operation.
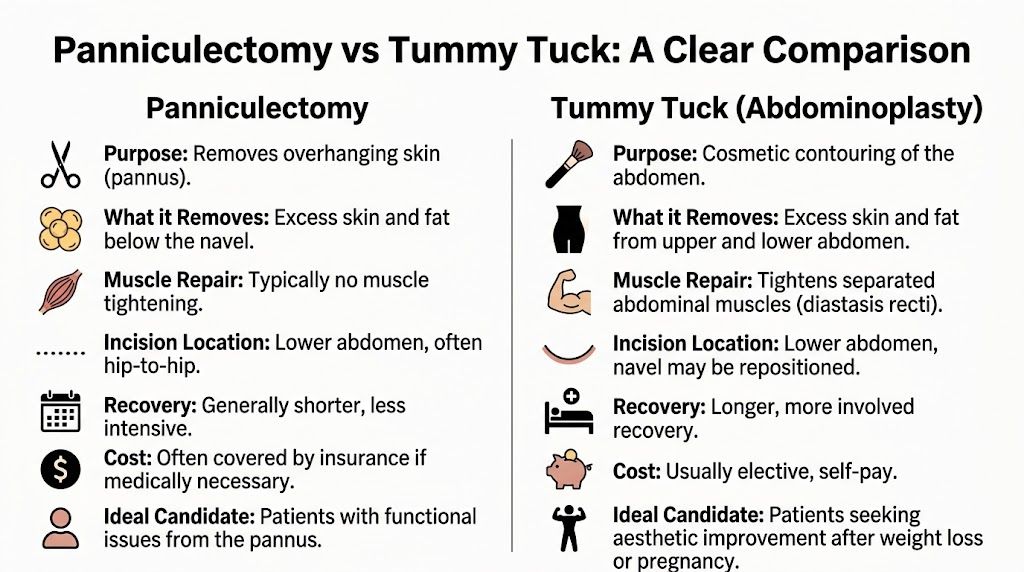
A panniculectomy removes excess hanging skin and fat in the lower abdomen. A tummy tuck, or abdominoplasty, is a cosmetic contouring procedure that usually does more. It often removes excess skin, improves the abdominal shape, and tightens separated abdominal muscles.
If you’re comparing the two in more depth, this overview of what is a tummy tuck procedure is a useful companion.
If your question is, “Will this remove the heavy apron that causes rashes and gets in the way?” you’re usually talking about panniculectomy.
If your question is, “Will this flatten my abdomen and tighten my muscles?” you’re usually talking about abdominoplasty.
The operations can involve similar lower abdominal incisions. Both remove tissue. Both change the contour of the midsection to some degree.
But the intent is different, and intent shapes everything else. Surgical planning. insurance. recovery expectations. scar placement. whether muscle repair is included.
| Feature | Panniculectomy | Abdominoplasty (Tummy Tuck) |
|---|---|---|
| Primary goal | Functional relief from an overhanging pannus | Cosmetic reshaping of the abdomen |
| What it removes | Excess lower abdominal skin and fat | Excess abdominal skin and fat, often more contour focused |
| Muscle tightening | Typically no | Usually yes |
| Focus of result | Less bulk, less pull, improved hygiene and comfort | Flatter, firmer, more sculpted abdomen |
| Insurance possibility | May be covered if medically necessary | Usually elective and self-pay |
| Best fit for | Patients with functional symptoms from hanging tissue | Patients seeking aesthetic improvement |
A panniculectomy does not usually include muscle plication. In the National Center for Biotechnology Information review, the procedure is described as removal of excess skin and subcutaneous tissue without the muscle tightening that distinguishes it from abdominoplasty: https://www.ncbi.nlm.nih.gov/books/NBK499822/
That one difference explains a lot.
Without muscle repair, a panniculectomy can solve the burden of overhanging tissue while leaving some abdominal fullness, upper abdominal laxity, or separation of the abdominal wall unchanged. For a patient seeking function first, that may be exactly right. For a patient focused on contour, it may feel incomplete.
When patients say, “I want the skin gone, but I also want my stomach tight again,” they may be describing goals that fit abdominoplasty better than panniculectomy.
Neither is better in the abstract. The better operation is the one that matches your problem.
Choose the wrong frame, and disappointment follows. A patient who needs functional relief may overpay for a cosmetic operation that wasn’t necessary. A patient who wants full contouring may choose panniculectomy and later realize it didn’t address muscle laxity.
That’s why good consultations spend as much time clarifying goals as examining anatomy.
Most patients feel less anxious once the operation becomes concrete. A panniculectomy follows a clear sequence, and each step has a reason.
On the day of surgery, your surgeon usually marks the abdomen while you’re standing. That helps map the tissue that needs to be removed and plan the final scar placement as accurately as possible.
You’ll also meet the anesthesia team. Panniculectomy is typically performed under general anesthesia, and the operation usually lasts 1 to 5 hours according to the National Center for Biotechnology Information surgical review: https://www.ncbi.nlm.nih.gov/books/NBK499822/
The usual incision is a transverse incision in the suprapubic crease. In plain language, that means a horizontal incision low on the abdomen, often in an area that can be covered by underwear or a swimsuit.
The dissection is carried through Scarpa’s fascia down to the abdominal wall muscles. Then the excess pannus is removed, and the remaining tissue is brought together for closure.
Here’s the core sequence:
Incision placement
The surgeon opens along the planned lower abdominal line.
Tissue elevation and dissection
The tissue is carefully separated along the appropriate plane to expose and mobilize the pannus safely.
Excision of the pannus
The overhanging skin and subcutaneous fat are removed.
Hemostasis
Bleeding is controlled carefully throughout the operation.
Layered closure
The incision is closed in several layers to reduce tension and support healing.
In large-volume cases, exposure can be difficult. The same NCBI surgical review notes that specialized retractors can reduce operative time by 30 to 50 percent by improving exposure and reducing tissue tension: https://www.ncbi.nlm.nih.gov/books/NBK499822/
That may sound technical, but the practical meaning is simple. Better exposure helps the surgeon see clearly, handle tissue more safely, and close with less strain on the wound edges.
After the tissue is removed, your surgeon will usually place drains. These collect fluid that would otherwise build up under the skin.
Many patients worry when they hear the word “drain.” In reality, it’s a routine part of surgery like this. Drains are used because removing a large amount of tissue leaves temporary space where fluid can collect.
Here’s a short visual explanation if seeing the process helps more than reading about it:
When you wake up, you can expect:
You may also be asked to walk early and gently. That early movement is part of safe recovery.
Most of the operation is not about making the abdomen look smaller. It’s about removing the weight and friction of tissue that your body no longer needs but still has to carry.
Recovery is easier when you know what’s normal. Most patients don’t struggle because recovery is impossible. They struggle because they didn’t expect the routine, the drains, or the uneven pace of healing.
The first result you usually notice is practical. The heavy apron is gone. Clothing fits differently. Cleaning the area is easier. Standing and walking can feel less cumbersome even while you’re still swollen.

This is the most hands-on phase.
You’ll be managing your incision, recording drain output, wearing a binder, and walking carefully. Patients typically keep drains for 7 to 14 days and wear a compression binder for 4 to 6 weeks, based on Cleveland Clinic’s panniculectomy guidance: https://my.clevelandclinic.org/health/procedures/panniculectomy
Common early experiences include:
This is often when patients feel much better, but still need restraint.
The same Cleveland Clinic guidance notes that 85% of patients see resolution of skin rashes within 6 weeks after surgery: https://my.clevelandclinic.org/health/procedures/panniculectomy
That’s an important point. The payoff isn’t only visual. For many people, this is when they realize they’re no longer fighting the same chronic skin irritation.
A few practical habits help during this phase:
For some patients, a more organized recovery plan makes a big difference. If you’re preparing for mobility challenges, gait changes, or a slow return to activity, this guide on personalized rehabilitation care after surgery offers practical ideas worth discussing with your care team.
Swelling improves gradually. Scars mature slowly. Your result becomes clearer over months, not days.
Cleveland Clinic also notes that with proper care such as silicone sheeting, scar hypertrophy risk can drop from 15% to under 5% over a 12-month maturation period, and binder use can speed edema reduction by 40%: https://my.clevelandclinic.org/health/procedures/panniculectomy
That tells patients two useful things. First, scar care matters. Second, your early result is not your final result.
Recovery after panniculectomy is often less about pain than about patience. The body improves in layers.
A good panniculectomy result usually means:
It may not mean a flat, sculpted stomach. If you keep that distinction clear, you’re more likely to be happy with the outcome.
Many patients find this frustrating. They assume that if a panniculectomy solves a medical problem, insurance will automatically approve it.
That’s often not how it works.
Coverage usually depends on whether the procedure can be documented as medically necessary, not helpful or desired. A pannus that causes chronic skin problems and hangs below the pubis fits that conversation far better than generalized dissatisfaction with abdominal appearance.
In the United States, initial insurance denial rates for panniculectomy can be as high as 60 to 70 percent, and medical necessity typically requires the pannus to hang below the pubis with at least 3 months of documented, treatment-resistant rashes or infections, according to this panniculectomy FAQ and insurance discussion: https://drjhopkins.com/blog/panniculectomy-frequently-asked-questions/
The phrase “documented” is the whole game.
Insurers often want evidence such as:
Many denials aren’t saying the patient has no real problem. They’re saying the file didn’t prove the problem in the specific way the insurer requires.
That’s why a careful paper trail matters more than patients expect.
If you think you may need insurance coverage, start documenting symptoms before your consultation, not after a denial.
Even when discussing insurance, it helps to understand the moving parts of surgical cost. A panniculectomy bill may involve:
Exact pricing varies by case, facility, and whether additional procedures are planned. If insurance covers part of the operation, those line items may still be handled differently depending on your policy.
For practical home planning after surgery, including equipment and comfort setup, this guide on recovering from surgery at home can help you think through the logistics before your procedure date.
If your first answer is no, that may not be the final answer. This article on does insurance cover plastic surgery helps clarify how medical necessity and coverage decisions often work.
A stronger appeal usually includes:
The most successful patients tend to approach insurance the way they’d approach any formal review. They don’t rely on a single sentence saying the procedure would be beneficial. They build a documented case.
Once you understand the procedure, the next decision is who should perform it. That choice affects safety, planning, communication, and whether your result matches your actual goals.
A panniculectomy may sound straightforward because it “just removes skin,” but large-volume tissue removal is not minor surgery. The surgeon has to judge candidacy carefully, manage wound-healing risk, coordinate anesthesia and facility safety, and be honest about what the operation will and won’t do.
Start with the essentials:
You also want a surgeon who can separate panniculectomy from abdominoplasty in a clear way. If the conversation gets blurry, patients often end up expecting the wrong result from the wrong procedure.
There’s real value in having your evaluation, surgery, and follow-up care close to home. Recovery after abdominal surgery involves multiple touchpoints. Questions come up. Dressings need review. Drains need management. Scars need monitoring.
For patients on Cape Cod, local access can make that whole process easier.
This aspect combines credentials and setting. Dr. Marc Fater of Cape Cod Plastic Surgery brings more than 30 years of experience, is a board-certified plastic surgeon, and operates in an on-site, AAAASF-accredited surgical suite. For a procedure like panniculectomy, those details matter because they speak to both judgment and safety.
A good consultation shouldn’t feel like a pitch. It should feel like a careful medical conversation. You should leave knowing whether you’re a candidate, whether your goals fit panniculectomy or another procedure, what risks need attention, and how recovery is likely to affect your daily life.
Yes, it can, and that’s common in practice. But combined surgery can raise risk. A large analysis found that adding panniculectomy to ventral hernia repair increased wound complications, reoperation, and overall morbidity compared with hernia repair alone: https://www.plasticsurgery.org/documents/medical-professionals/quality-resources/Measure-Specifications-Abdominoplasty-Panniculectomy.pdf
The removed tissue is gone permanently, but your long-term result still depends on weight stability. Significant weight regain can change the abdominal contour again.
Yes. You should expect a lower abdominal scar. The tradeoff is that the scar replaces a heavy overhang that may be causing daily symptoms. Most surgeons consider scar placement and tension very carefully, but no honest surgeon will promise an invisible scar.
No. It’s primarily a functional procedure for patients whose pannus causes hygiene problems, skin irritation, or mobility issues. It may improve appearance, but that isn’t its main purpose.
If you’re wondering whether a panniculectomy is the right next step after weight loss, a consultation can give you a clear answer. Cape Cod Plastic Surgery offers patients on Cape Cod access to expert evaluation, thoughtful surgical planning, and experienced care from Dr. Marc Fater in an accredited surgical setting.
Considering skin tightening after liposuction? Explore recovery, influencing factors, and effective treatment options, from non-invasive to surgical.

July 8, 2026
The Gold Standard in Plastic Surgery: Why Board Certification Matters

July 7, 2026
Our 2026 guide explains precisely how does botox work. Discover its science, procedure, benefits, and risks in simple terms to see if it's for you.
Cape Cod Plastic Surgery offers expert cosmetic and reconstructive procedures in a safe, accredited setting. Led by Dr. Marc Fater, we combine advanced techniques with personalized care to help you look and feel your best.
Monday: 9:00 AM – 5:00 PM
Tuesday: 9:00 AM – 5:00 PM
Wednesday: 9:00 AM – 5:00 PM
Thursday: 9:00 AM – 5:00 PM
Friday: 9:00 AM – 5:00 PM