
Split Earlobe Repair: What to Expect from Start to Finish
Considering split earlobe repair? Learn about causes, techniques, costs, healing, and how to choose a qualified surgeon for natural-looking results.
Apr 26, 2026

You’re taking off mascara, leaning toward the mirror, and suddenly you see it. A gap in the lash line. Maybe it’s just a few lashes. Maybe it’s enough that your eye looks different. A common immediate thought is: will my eyelashes grow back?
That question usually comes with a second feeling. Worry. If you’ve recently used lash extensions, rubbed your eyes during allergy season, gone through a stressful period, or noticed changes as you’ve gotten older, it’s easy to assume the worst.
The reassuring answer, in most cases, is yes. Eyelashes usually do grow back. The timeline depends on why they were lost, whether the follicle is still healthy, and whether an underlying issue is slowing the normal cycle. For many patients, the missing piece isn’t effort. It’s understanding what’s normal, what isn’t, and when age, hormones, or nutrition may be subtly changing the pace of regrowth.
A patient will often tell me the same story in slightly different words. “I wasn’t looking for a problem. I just noticed my lashes seemed uneven one morning.” That’s how it starts for many people. A bare spot near the outer corner. A lash curler incident. Thinning after extensions. Sparse regrowth after chemo. Or lashes that seem slower to return than they did years ago.
That reaction is understandable. Eyelashes do more than frame the eye. They’re tied closely to how rested, youthful, and healthy you look. When they thin, patients don’t just notice a cosmetic change. They worry something is wrong.
Missing lashes can feel dramatic because the change is so close to the center of your face.
The good news is that most lash loss is temporary when the follicle remains intact. Natural shedding, minor mechanical trauma, and many temporary medical stressors allow lashes to return over time. What creates confusion is that regrowth isn’t instant, and it rarely happens all at once. One part of the lash line may fill in while another still looks sparse.
That unevenness leads many people to think the lashes aren’t returning, when in fact they’re moving through a normal cycle at different speeds.
A few missing lashes after makeup removal is very different from ongoing thinning, bald patches, eyelid irritation, or slow return over many months. I’m especially careful with patients over 40, because hormonal shifts and nutritional deficiencies can make a simple lash loss problem look more persistent than expected.
If you’re asking “will my eyelashes grow back,” the key question is often this: what caused the loss, and is anything interfering with regrowth now?
Lashes follow a rotating schedule, not a single reset point. That is why one part of the lash line can look fuller while another still appears sparse, even when the follicles are functioning normally.
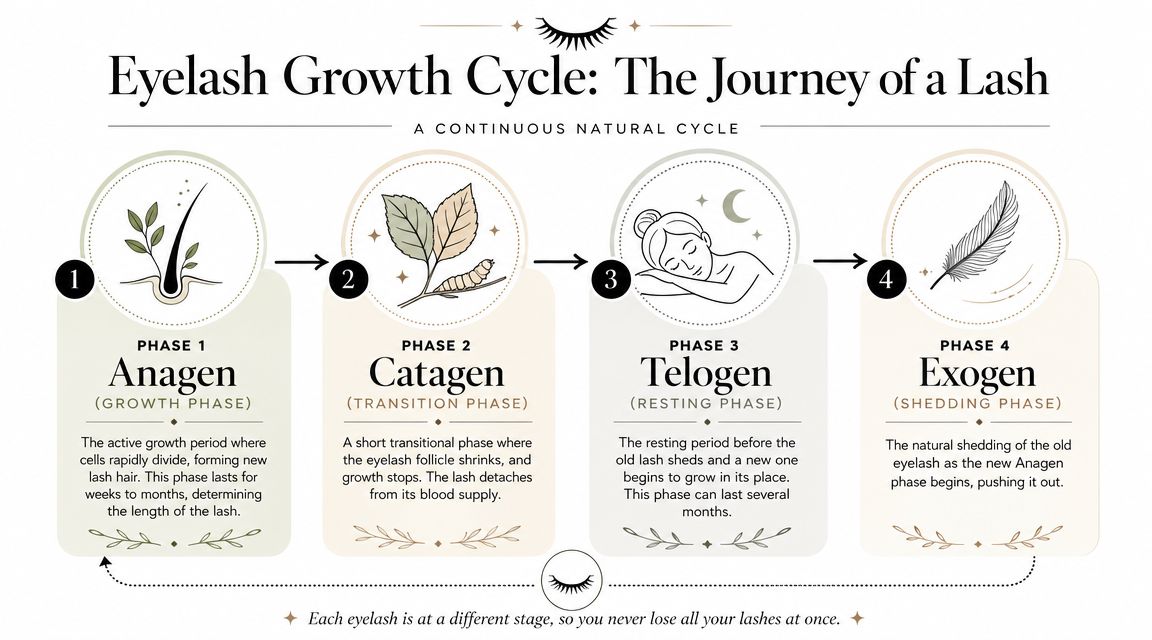
A useful way to understand this is to picture each follicle as operating on its own clock. One lash is actively growing. Another has stopped growing and is holding steady. A third is resting before it sheds. Because these clocks are staggered, regrowth rarely looks even from week to week.
According to Dr. Bittel’s medical overview of eyelash regrowth, lashes often return within about 6 to 12 weeks when the follicle remains healthy. That same overview notes that the growth phase lasts several weeks, lashes grow slowly each day, and only a portion of upper lashes are actively growing at a given time. For patients, the practical takeaway is simple. Slow, uneven return can still be normal.
This is the active growth phase. The follicle is building the lash fiber much like a hair factory that is fully switched on. If a lash is lost during this phase, replacement can take longer because that production cycle has been interrupted.
This is the transition phase. Growth stops, and the follicle briefly changes from production mode to a resting state. It is short, but it helps explain why lashes do not keep lengthening indefinitely.
This is the resting phase. The lash stays in place until it sheds, and a new lash begins to develop in its own timing. That staggered turnover is what keeps the lash line from disappearing all at once.
A few lashes on a cotton pad or pillowcase can be completely normal.
Healthy lids carry many lashes, so small daily shedding often goes unnoticed. If a lash falls out at the end of its natural cycle, regrowth is usually more straightforward than if it was pulled out by rubbing, extensions, or a curler accident. In those situations, the follicle may need more time to recover before it starts producing a strong new lash.
This is one place where age can change the picture. In patients over 40, the cycle may feel slower because hormonal shifts and low iron, low protein intake, or other nutrient gaps can reduce how efficiently follicles return to active growth. Stress can add another layer, and these practical tips for hair restoration help explain why recovery is sometimes slower after illness, emotional strain, or physical stress.
If your lashes are shedding a little but the skin of the eyelid looks healthy, that often fits a normal cycle. If regrowth stays sparse, becomes patchy, or seems much slower than it used to be, the issue is often not the lash alone. It may be the follicle’s environment, which is why a closer medical evaluation can be so helpful.
When lashes thin, the cause usually falls into one of three groups. The first is mechanical damage, meaning something physically stressed the lash or follicle. The second is medical disruption, where inflammation, illness, or a skin condition interferes with normal growth. The third is systemic stress, such as major illness or treatment.

This category is common and often overlooked because the habits feel harmless.
The pattern here is usually patchy or uneven. One area may look sparse while another seems normal.
Medical conditions can interrupt the lash cycle to a greater extent. According to NVISION’s review of eyelash loss causes, medical conditions can significantly disrupt eyelash growth, and hormonal imbalances like thyroid disease or chronic stress can prolong recovery to months or even over a year. The same source notes that after chemotherapy, lashes typically regrow in weeks to months, and infections can delay recovery for weeks to months after treatment.
A few medical possibilities include:
If the lid is red, irritated, crusted, itchy, or tender, I think less about cosmetics and more about inflammation or skin disease.
Ongoing lash loss with itching or eyelid scaling deserves an exam, not a stronger mascara.
Chemotherapy is the clearest example, but it isn’t the only one. Major stress, illness, and hormonal shifts can all disrupt how follicles behave. Some patients benefit from broader hair health support while they address the trigger. If stress-related shedding may be part of the picture, these practical tips for hair restoration can help you think through daily habits that support recovery.
The important point is this. The lash line often reflects what’s happening in the rest of the body.
This is the area that generic lash advice often misses. A younger patient and a post-menopausal patient may lose lashes for the same reason, yet heal on very different timelines. If you’re over 40 and asking why your lashes aren’t coming back the way they used to, age-related hormone changes and nutrient status deserve attention.

Hair follicles respond to the body’s internal environment. Estrogen shifts, thyroid changes, stress hormones, and reduced nutritional reserve can all make the lash cycle less predictable. According to Medical News Today’s discussion of lash regrowth factors, post-menopausal women can experience a 30 to 50% longer disruption to the anagen phase due to estrogen decline, extending regrowth to 4 to 6 months. The same source states that correcting deficiencies in nutrients such as biotin and iron can lead to a 70% improvement in lash density within 3 months for affected individuals.
That doesn’t mean every patient over 40 will have slow lash return. It means age can shift the baseline.
Lashes are small, but follicle biology is demanding. When protein intake is poor, iron is low, or a patient isn’t absorbing nutrients well, the body may prioritize more important systems first. Hair, skin, and nails often reveal that imbalance.
For some patients, reviewing diet is useful. If increasing protein is part of your plan, this guide to clean protein from Maximum Health offers practical ideas for people trying to avoid common dietary triggers while supporting hair health.
A broader health review also matters before any aesthetic procedure. Patients who are already thinking about nutrition and healing may also find our guidance on taking vitamin C before surgery helpful when considering how supplementation fits into medical care.
If you’re noticing the following, a personalized evaluation makes sense:
This overview gives a helpful visual explanation of how regrowth can vary:
For patients over 40, this is often the turning point. The problem isn’t always the lash itself. It’s the environment the follicle is trying to grow in.
A common scenario in my office is a patient who says, “I stopped the extensions months ago, so why are my lashes still thin?” That question matters even more after 40, when the follicle is often recovering in a different hormonal and nutritional environment than it did a decade earlier. Treatment works best when we match the option to the biology, not just to the symptom you see in the mirror.
Some lashes need protection while the follicle completes its normal cycle. Others respond to prescription treatment that keeps lashes in the active growth phase longer. If age-related hormonal shifts, low iron, low protein intake, or other deficiencies are slowing the follicle down, regrowth may be less dramatic until those issues are addressed.
If lash loss followed rubbing, harsh makeup removal, or repeated extensions, the first job is to stop giving the follicle the same injury over and over. I usually recommend gentle cleansing, a pause from adhesives and curlers, and less manipulation at the lid margin. Follicles recover best in a calm environment.
Supportive products can play a role, but they should not distract from the bigger picture. For patients asking how structural support fits into hair health more broadly, this ultimate guide to collagen for hair offers a helpful overview.
The best-known prescription option for eyelash enhancement is bimatoprost, sold as Latisse. It works by prolonging the growth phase, which can help lashes grow longer, darker, and fuller over time. Improvement is gradual. Patients usually need steady use and patience.
For patients who are curious about how this same medication performs in nearby hair-bearing areas, our article on whether Latisse works for eyebrows gives additional perspective.
A practical way to understand this is to picture the follicle as a tiny factory. If the factory is intact, a prescription product may help it stay open longer each cycle. If the factory is inflamed, scarred, or running short on raw materials such as iron or protein, the result is often slower and less complete. That is one reason expert evaluation becomes more useful with age.
| Treatment | How It Works | Typical Results Timeline | Best For |
|---|---|---|---|
| Gentle at-home care | Reduces friction and helps prevent further breakage | Gradual, depends on the natural lash cycle | Recent cosmetic or mechanical damage |
| Peptide-based lash serums | Conditions existing lashes and may support a healthier appearance | Changes may take weeks | Mild thinning and patients who want a non-prescription option |
| Latisse | Prolongs the active growth phase of the lash cycle | Gradual improvement with consistent use | Patients with intact follicles who want a prescription treatment |
| In-office regenerative approaches | Supports follicle health in selected cases | Varies by patient and protocol | Patients who need a more specific plan |
| Eyelash transplantation | Surgically places donor hairs in the lash line | Longer recovery and ongoing trimming or styling | Advanced or long-standing lash loss in selected candidates |
A patient with short-term extension damage usually needs a different plan than someone with persistent thinning after menopause, thyroid change, or a period of poor nutrition. A patient with eyelid inflammation may not improve until that irritation is treated first. A patient with true follicle injury may need to discuss reconstructive options rather than waiting month after month for regrowth that is unlikely to come.
Generic lash advice often falls short for patients over 40. The question is not only, “What product should I use?” It is also, “Is my follicle still healthy, and is my body giving it what it needs to grow?” That answer often determines both the timeline and the final result.
Patients are often relieved to learn that an eyelash consultation is straightforward. You sit down, describe what changed, and we begin with the history. Did the thinning happen suddenly or gradually? Was there recent stress, surgery, extensions, irritation, menopause, illness, or a new medication? Are the brows affected too?

I examine the lid margin, skin quality, follicle pattern, and whether the loss appears mechanical, inflammatory, or systemic. The details matter. A clean sparse patch suggests one pathway. Redness, scaling, and irritation suggest another.
We also talk about goals. Some patients want to restore what they had before. Others want a fuller cosmetic result than nature gave them. Those are different conversations, and they lead to different options.
An effective plan may include watchful waiting, prescription therapy, changes in cosmetic habits, treatment of an eyelid condition, or discussion of a more advanced solution when loss appears long-standing. For patients already considering facial rejuvenation, eyelid position and upper-lid skin can also affect how noticeable lash thinning appears. That’s one reason some patients also explore eyelid surgery and blepharoplasty for a more youthful look.
The best consultation doesn’t just answer whether lashes can grow back. It explains why they were lost and what will give you the safest path forward.
This is especially true for patients in midlife and beyond. If hormones, thyroid function, iron status, or stress are part of the story, treating the lash alone won’t always give the result you want. A careful evaluation keeps you from wasting time on products that don’t match the underlying problem.
A common scene in my office is a patient leaning toward the mirror and saying, “I thought they would be back by now.” That concern is understandable. Eyelash regrowth is often possible, but the timeline depends on why the lashes were lost, whether the follicle is still healthy, and, for many patients over 40, whether age-related hormone shifts or nutrient deficiencies are slowing the process.
Usually, yes, if the eyelid skin is comfortable and you remove makeup gently. New lashes are delicate, much like short new hairs after a haircut. They can break more easily with waterproof mascara, vigorous rubbing, or daily tugging at the lash line.
If your lash loss started after irritation, blepharitis, or an allergic reaction, give the lid margin time to settle before returning to a full cosmetic routine. A simpler approach often helps the follicle recover without more friction.
Often, yes. The first round of regrowth may look finer, lighter, or slightly less uniform. That can happen because the follicle is restarting its cycle, not because recovery has failed.
For patients in midlife, the answer is a little more nuanced. Estrogen declines, thyroid changes, and shifts in androgen balance can all affect hair caliber and growth speed, including at the lashes. In that setting, lashes may return more slowly or look less dense unless the underlying issue is addressed.
Normal shedding is quiet. You may notice an occasional lash on your cheek or pillow, while the lash line still looks generally even.
A true problem is more likely if you see visible gaps, thinning that continues for weeks, lids that itch or burn, scaling at the base of the lashes, or loss that seems out of proportion to your beauty routine. I also pay close attention when patients describe a gradual change with no obvious trigger, especially after 40. That pattern can point to low iron, low vitamin D, protein deficiency, thyroid imbalance, or hormonal change rather than simple shedding.
They usually do if the follicle was stressed but not scarred. Extensions can act like repeated traction on a small anchor point. If enough pull is applied over time, the lash may shed before it was ready.
Recovery often feels slow because lashes do not all regrow at once. Each follicle follows its own schedule. If extensions were combined with glue irritation or chronic inflammation, regrowth may take longer and deserves closer evaluation.
Castor oil can condition the lashes and make them look glossier. It is not the same as a treatment that has been studied for stimulating lash growth.
That distinction matters. If your lashes are sparse because of menopause-related hormone shifts, iron deficiency, thyroid disease, or eyelid inflammation, oil alone usually will not solve the problem. It may also irritate sensitive eyes, so use caution.
Only if a deficiency is part of the reason they thinned. Hair follicles are like tiny factories. They need adequate raw materials to build a healthy lash shaft, including protein, iron, and certain vitamins. If those materials are in short supply, the factory slows down.
For patients over 40, this is often overlooked. Restrictive dieting, low ferritin, poor protein intake, vitamin D deficiency, and borderline B12 levels can all affect regrowth without causing dramatic symptoms elsewhere. Taking random supplements is rarely the best first step. A targeted evaluation is much more useful.
Schedule an evaluation if lash loss is patchy, prolonged, associated with redness, crusting, tenderness, or follows a major health change. Seek help if you have had repeated extension use, a history of thyroid disease, recent menopause, unexplained hair thinning elsewhere, or lashes that return weaker each cycle.
I am especially cautious when a patient says, “My lashes just do not grow the way they used to.” That statement often points to more than cosmetics. It suggests a biologic change worth identifying so treatment can match the cause, rather than relying on trial and error.
If you’re worried about thinning lashes and want clear answers from an experienced surgeon, Cape Cod Plastic Surgery offers personalized guidance to help determine why your lashes changed and which treatment options make sense for your goals.
Considering split earlobe repair? Learn about causes, techniques, costs, healing, and how to choose a qualified surgeon for natural-looking results.

July 24, 2026
Explore laser skin rejuvenation in 2026, including ablative vs non-ablative options, recovery, risks, and how to choose a provider.

July 23, 2026
Understand your surgical drain removal. Our patient guide covers home care, the procedure, and what to expect in 2026. Get expert info from Cape Cod Plastic
Cape Cod Plastic Surgery offers expert cosmetic and reconstructive procedures in a safe, accredited setting. Led by Dr. Marc Fater, we combine advanced techniques with personalized care to help you look and feel your best.
Monday: 9:00 AM – 5:00 PM
Tuesday: 9:00 AM – 5:00 PM
Wednesday: 9:00 AM – 5:00 PM
Thursday: 9:00 AM – 5:00 PM
Friday: 9:00 AM – 5:00 PM