Breast Augmentation vs Fat Transfer: A Patient Guide
Breast augmentation vs fat transfer explained honestly. Compare results, recovery, cost, candidacy, and mammogram impact to choose with confidence.
Apr 27, 2026

You may be reading this after another day of shifting your bra straps, rubbing sore shoulders, adjusting your posture, and wondering whether this is just something you’re supposed to live with. Maybe exercise feels uncomfortable. Maybe rashes keep coming back under the breast fold. Maybe getting dressed is frustrating because nothing fits the way it should.
If that’s where you are, it helps to hear this clearly. Wanting relief from heavy, painful breasts is not shallow, and it isn’t “just cosmetic” because someone else says so. For many patients, breast reduction is about function, comfort, skin health, sleep, movement, and getting through the day without constant physical reminders that something is wrong.
The hard part is that insurance rarely sees your lived experience unless it’s translated into paperwork. That’s why breast reduction requirements for insurance can feel so maddening. You know what your body is doing. The insurer wants records, measurements, failed treatments, symptom notes, codes, photos, and a medical argument.
The good news is that this process is usually more manageable once you stop thinking of it as a mystery and start treating it like a case file. Every appointment note, every physical therapy record, every photo, and every surgeon measurement becomes evidence. When the file is strong, the insurer has a clearer basis to say yes.
A patient often starts in the same place. She’s been dealing with neck tension for years, has deep marks from bra straps by the afternoon, avoids high-impact exercise, and keeps trying to “make it work” with better bras or pain relievers. She may even delay a consultation because she assumes insurance won’t help.
That assumption isn’t always right.
Breast reduction can qualify for coverage when it’s documented as treatment for symptomatic macromastia, not merely a preference for smaller breasts. Insurance companies look for evidence that breast size is causing real physical problems and that less invasive options haven’t solved them. The challenge isn’t only having symptoms. The challenge is proving them in a way the insurer recognizes.
Think of the process like assembling a travel packet for an important trip. If you show up with only part of what’s needed, you get delayed. If you bring the full packet, organized and complete, the path gets much smoother. Insurance works much the same way.
A strong submission usually includes four things working together:
Breast reduction approval is rarely about one dramatic complaint. It’s usually about a consistent pattern of symptoms documented over time.
When patients approach the process this way, the insurance maze starts looking less like a wall and more like a sequence of solvable tasks.
Insurance companies make one basic distinction that shapes the entire process. They separate procedures they view as cosmetic from procedures they view as medically necessary. If a breast reduction is framed as appearance-driven, coverage usually won’t follow. If it’s framed and documented as treatment for a medical condition, the conversation changes.

The simplest way to understand medical necessity is to think like a lawyer preparing a case. The insurer is the reviewer. Your records are the evidence. The surgeon’s note is the argument tying everything together.
The insurer wants proof of three things:
For breast reduction, the medical problem is usually breast hypertrophy or symptomatic macromastia. The symptoms that often matter most are chronic back, neck, and shoulder pain, skin irritation or recurrent rashes under the breasts, bra strap grooving, and limits on exercise or daily activity. Some patients also report numbness, posture strain, or repeated skin breakdown.
Patients often feel confused here, and understandably so. If you hurt every day, it seems obvious that treatment is needed. But insurance reviewers usually don’t meet you. They only see records. If your chart just says “wants breast reduction” and doesn’t spell out the pain pattern, duration, physical findings, and failed treatments, the reviewer may label the request incomplete.
That’s why conservative care matters so much.
Insurers often want to see that you’ve already tried non-surgical measures first. According to GoodRx’s overview of breast reduction insurance requirements, insurers mandate 3-6 months documented failure of conservative therapies, and qualifying symptoms include chronic back, neck, and shoulder pain, shoulder grooving, and recurrent intertrigo. The same source notes that plans such as UnitedHealthcare, Anthem, and Moda Health require physician letters and medical records showing that surgery is the remaining effective option.
A strong chart usually shows a pattern, not a single complaint. That pattern might include repeated visits for upper back pain, a dermatology note about recurrent rash, physical therapy records showing limited relief, and your surgeon’s exam documenting bra strap indentation and breast-related discomfort.
Useful records often include:
Practical rule: Don’t ask your doctors to write that you “want smaller breasts.” Ask them to document what your breasts are doing to your body.
This distinction matters more than many patients realize. Cosmetic language focuses on size preference, shape, clothing fit, or appearance. Medical language focuses on pain, skin injury, posture, restricted activity, and treatment failure.
That doesn’t mean appearance concerns aren’t real. It means they don’t usually help the insurance case.
If you want a broader primer on how insurers classify procedures, this guide on whether insurance covers plastic surgery is a useful companion. It helps put breast reduction into the larger insurance framework.
The easiest way to manage breast reduction requirements for insurance is to stop seeing them as random requests and start organizing them into four evidence pillars. Each one answers a different insurer question. When one pillar is weak, denials become more likely. When all four line up, the submission feels much more credible.
This is the backbone of the file. The insurer needs to see that your symptoms are persistent, not occasional.
Good documentation might show repeated complaints about upper back pain, neck strain after work, shoulder grooves from bras, exercise limits, or recurring rash under the breasts. It helps when records show how these symptoms affect ordinary life. Trouble sleeping comfortably, avoiding cardio, needing frequent pain medication, or changing bras multiple times a day because of discomfort are all relevant when documented by a clinician.
A symptom timeline gets stronger when records come from more than one source, such as a primary care physician, physical therapist, chiropractor, dermatologist, or orthopedist.
Insurance companies often want evidence that surgery isn’t the first step. They want to see what you already tried.
That might include:
The key isn’t just listing these attempts. The key is showing that they didn’t provide enough lasting relief.
If a reviewer can’t see what failed, they may assume surgery was requested too early.
The clinical case becomes precise as your plastic surgeon documents physical findings, symptoms, breast size in relation to your body, and how much tissue is expected to be removed.
One major concept here is the Schnur Sliding Scale. As explained in this review of insurance weight requirements for breast reduction, the Schnur Scale is a benchmark used by insurers such as Blue Cross Blue Shield. It links body surface area, or BSA, with a minimum amount of tissue removal to support medical necessity. For example, a patient with a BSA of 1.35 m² might need at least 260 grams resected per breast, and meeting these gram thresholds was associated with a 90% approval rate in the original study.
Many patients find this aspect confusing, assuming approval depends only on pain. In some policies, symptom documentation is central. In others, symptom documentation must also align with predicted tissue-removal thresholds. Your surgeon’s estimate matters because the insurer may compare that estimate against its own policy language.
Medical photos aren’t glamour shots. They’re clinical evidence. They help demonstrate breast size, shoulder grooving, skin issues, posture effects, and overall anatomy relevant to surgery planning.
The insurer may also require a formal letter of medical necessity. This letter usually ties the whole file together by explaining:
If your records are being transmitted between offices, use secure processes. Even simple administrative tools matter. A clear HIPAA-compliant fax cover sheet can help protect patient information and reduce delays when records move between a primary care office, therapist, dermatologist, and surgical practice.
| Document/Evidence Type | What It Proves | Who Provides It |
|---|---|---|
| Symptom history in office notes | Your pain, rash, grooving, or activity limits are ongoing and medically recognized | Primary care clinician or specialist |
| Conservative treatment records | You tried non-surgical options before requesting surgery | Physical therapist, dermatologist, prescribing clinician, other treating providers |
| Plastic surgery consultation note | Clinical findings, anatomy, symptoms, and surgical plan support medical necessity | Plastic surgeon |
| Height, weight, and BSA calculation | Insurer can compare your body measurements to policy criteria | Plastic surgeon |
| Estimated tissue removal | Planned resection may meet insurer thresholds such as Schnur-related criteria | Plastic surgeon |
| Medical photographs | Visual support for hypertrophy, asymmetry, grooving, or skin changes | Plastic surgery office |
| Letter of medical necessity | A clear medical argument connecting symptoms, findings, and procedure | Plastic surgeon |
| Insurance card and policy details | Ensures the request is submitted under the correct plan and rules | Patient and surgical office |
A strong file tells one consistent story. The pain notes match the physical therapy notes. The rash history matches the photos or dermatology records. The surgeon’s estimate matches the insurer’s technical standard. Nothing feels disconnected.
That consistency matters more than patients often realize. Insurance reviewers are looking for gaps. Your job is to leave as few as possible.
Patients usually feel better once they know what happens in what order. Preauthorization has waiting periods, paperwork handoffs, and occasional detours, but the overall path is fairly predictable when the office is organized.
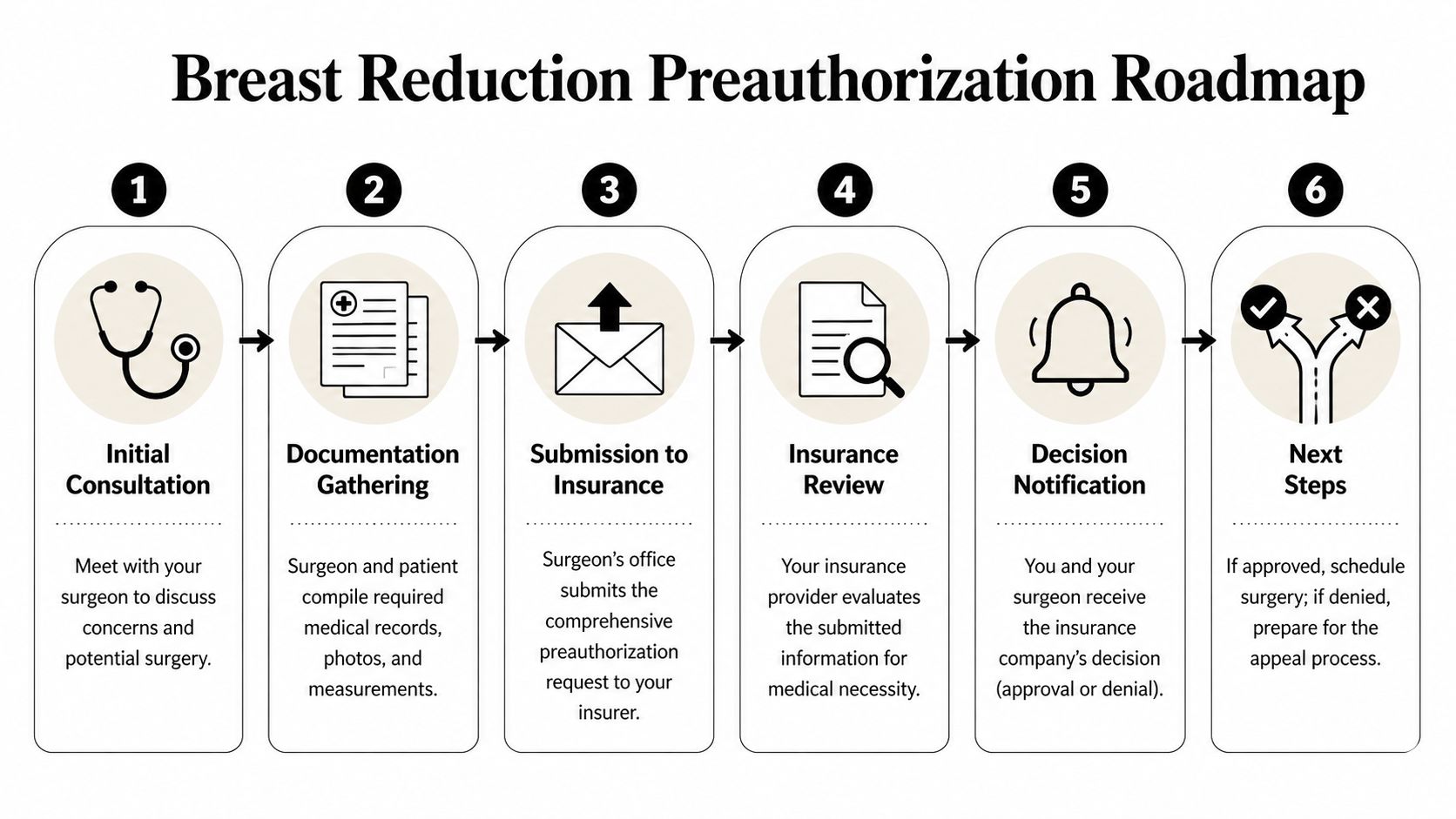
This visit is where the file starts taking shape. You describe symptoms, prior treatments, and goals. The surgeon examines you, reviews whether your symptoms fit a medical-necessity pattern, and notes whether your plan may require more records before submission.
If you want to arrive prepared, this guide to what happens at an initial plastic surgery consultation can help you know what to bring and what questions to ask.
After the consult, the office may request records from your primary care physician, therapist, chiropractor, dermatologist, or other treating clinicians. This stage often feels slow because outside offices don’t all send records at the same pace.
This is also when medical photos, measurements, diagnosis coding, and the surgeon’s letter are finalized. Some offices can submit quickly. Others may wait until missing records arrive so the packet is stronger the first time.
Once the packet is complete, it goes to the insurer for prior authorization or preauthorization review. If that term has always felt abstract, it helps to understand prior authorization effectively before you start. The basic idea is simple. The insurer reviews the request before surgery and decides whether it meets the plan’s medical-necessity standards.
At this stage, details matter. According to this summary of breast reduction insurance trends, approximately 65% of breast reduction procedures involve insurance coverage, with 28% fully covered and 37% partially covered. The same source notes that denial rates rose from 18% in 2012 to 41% in 2017, with an overall average denial rate of 28%. Common denial reasons included inadequate documentation at 39% and failure to meet medical criteria.
That’s why a rushed submission is rarely worth it.
A preauthorization packet should read like one clear story told by multiple records, not a pile of unrelated paperwork.
The insurer may approve the request, ask for more information, or deny it. Sometimes the reviewer wants clarification about tissue estimates, treatment history, photographs, or symptom duration. In some cases, the surgeon may speak directly with the insurer’s medical director in a peer-to-peer review.
This waiting period is often the hardest part emotionally because patients feel stuck. It helps to remember that silence doesn’t always mean trouble. It often means the file is in queue or under clinical review.
Three outcomes are common:
A denial is disappointing, but it doesn’t automatically end the process. Often it means one piece of the case file wasn’t documented in the way that specific insurer required.
Meeting the minimum requirements is one thing. Building a convincing insurance case is another. Patients who take an active role often make the process smoother because they help create a cleaner, more complete record from the start.
A simple notebook or phone note can be surprisingly useful. Record where the pain is, when it flares, what activities trigger it, and what you had to stop doing because of it. Note when rashes occur, when bra straps leave deep marks, and whether over-the-counter treatments helped.
You’re not creating evidence for the insurer directly. You’re creating memory support so your doctor visits are more precise. Precise visits usually lead to better chart notes.
Many charts are too vague because patients describe the problem generally and the note ends up general too. Instead of saying “my breasts bother me,” say where the pain is, how often it happens, what you’ve already tried, and what daily activities are affected.
Specificity helps with notes such as:
One of the most practical steps you can take is calling your insurance company and asking for the written medical policy for reduction mammaplasty or breast reduction. Policies vary more than patients expect.
According to this overview of policy variability among major insurers, requirements differ significantly across carriers such as UnitedHealthcare, Aetna, and Anthem. Aetna often requires patients to be 18+, while other policies may apply BMI rules or require 6-12 months of specialist reports. That variation is why a friend’s approval story may not match your plan at all.
For insurance cases, documentation quality matters almost as much as surgical planning. An experienced office knows how to connect symptoms, physical findings, photos, measurements, and treatment history into one coherent submission.
One option patients in Massachusetts often consider is Cape Cod Plastic Surgery’s overview of breast reduction benefits, which also helps patients think through whether their symptoms and goals fit a medically driven consultation. The key is finding a practice that treats preauthorization as a clinical process, not just an administrative task.
Case-building mindset: Don’t wait for the insurer to tell you what’s missing. Try to anticipate the weak spots before the file is submitted.
A reviewer who has never met you will ask simple questions. Are the symptoms documented? Did conservative treatment fail? Does the surgeon’s estimate match policy requirements? Do the photos support the written story?
If you can answer yes to all four, your file is in much better shape.
A denial feels personal, but it usually isn’t. Most denials mean one of two things. Either the insurer believes the file is missing evidence, or the request didn’t line up closely enough with that policy’s rules.

The first step is slow and boring, but it matters. Read the denial notice carefully and look for the exact reason given. It may say the predicted tissue removal was insufficient, the conservative treatment history was not documented clearly enough, the photos were inadequate, or the request did not meet the plan’s definition of medical necessity.
That reason tells you what the appeal needs to fix.
If the denial says documentation was incomplete, gather more treatment records. If it says symptom history was insufficient, ask the treating clinicians to clarify frequency, duration, and impact. If it says the insurer needs additional proof of skin issues, dermatology records may help.
Many offices also request a surgeon addendum or revised letter of medical necessity that directly responds to the denial language.
A denial letter is often less a verdict than a map to the missing piece.
Some patients find it helpful to review a broader B2B resource for denied insurance claims so they understand the logic of appeals and the importance of matching the appeal to the stated denial reason.
In some cases, the surgeon can speak directly with the insurance medical director. This conversation is often called a peer-to-peer review. It gives the surgeon a chance to explain the clinical picture in plain terms and answer questions that weren’t clear from the paperwork alone.
That doesn’t guarantee reversal, but it can help when the dispute involves medical judgment rather than a missing form.
A short video can also make the appeal process feel less abstract:
A strong appeal is direct. It should answer the insurer’s stated reason for denial and attach the records that solve that problem. It shouldn’t just repeat the original packet without changes.
If you appeal, keep copies of everything. Save the denial letter, appeal letter, fax confirmations, uploaded documents, and names of anyone you speak with. Organized patients often feel more in control, and that matters during a stressful process.
The insurance side of breast reduction works best when the clinical team and the patient are building the same file together. That means the practice isn’t only planning surgery. It’s also translating symptoms, findings, and treatment history into insurer language.
Dr. Marc Fater and his team evaluate the physical issues insurers commonly care about, such as breast-related pain patterns, skin irritation, shoulder grooving, and how those symptoms fit a medically necessary reduction request. During consultation and follow-up, the office can gather the measurements, clinical notes, and medical photographs that typically form the core of a submission.
That support matters because a surgeon’s office sees the difference between a chart that merely lists complaints and a chart that supports approval. The stronger version is usually more specific. It connects the patient’s symptom history to physical findings and to the planned amount of tissue removal.
Administrative follow-through matters too. A breast reduction request often requires record collection from outside clinicians, communication with the insurer, and response to requests for additional information. When an office is used to working through preauthorization, that process tends to be more organized and less confusing for the patient.
If a payer asks for clarification or issues a denial, the same file can often be strengthened with added records, clearer physician language, or a formal appeal. That kind of continuity helps because the people handling the appeal already understand the clinical story, the documentation trail, and the insurer’s concerns.
The practical value for patients is simple. You don’t have to guess what belongs in the file or try to decode insurer language alone. You still play an important role by reporting symptoms clearly and keeping records, but the office helps shape those details into a submission that makes medical sense on paper.
It depends on the plan. Some insurers include BMI-related rules or expect patients to attempt weight-related conservative measures first. Others focus more heavily on symptoms, documentation, and predicted resection weight. The most useful move is to get your policy’s written criteria and compare them with your surgeon’s evaluation rather than relying on general internet advice.
Policy language matters a lot. Some plans exclude cosmetic breast reduction but still allow coverage for medically necessary reduction mammaplasty under specific conditions. The question isn’t just whether the word “cosmetic” appears. The question is whether the policy also contains medical-necessity criteria for symptomatic macromastia, breast hypertrophy, or reduction mammaplasty.
Possibly, yes. According to this guide to insurance coverage after significant weight loss, insurers may still approve breast reduction if medical necessity persists and is well documented. In these cases, patients usually need to show that symptoms such as back pain and rashes continue despite a stable weight for 6-12 months, along with photos showing persistent hypertrophy and a surgeon’s letter confirming that the planned tissue removal still meets Schnur-related criteria.
That depends on the insurer. Some authorizations remain valid for a limited window, and the approval letter usually states the relevant dates or service period. Always read the approval notice carefully and ask the office to confirm scheduling deadlines so the authorization doesn’t expire before surgery is booked.
Because insurance approval doesn’t depend only on suffering. It depends on whether your file matches the language and standards of your specific plan. Many patients with legitimate symptoms still need stronger records, longer documented treatment history, or clearer surgeon estimates before a payer will approve the request.
Usually not. A consultation can help identify missing pieces early. If you’re short on documentation, the surgeon can often tell you what records to gather and what treatment history needs better support before submission.
If you’re dealing with persistent back, neck, or shoulder pain, skin irritation, or daily limits caused by heavy breasts, a consultation can help you understand whether your symptoms may support insurance coverage. Cape Cod Plastic Surgery works with patients to evaluate medical necessity, organize supporting documentation, and clarify the next steps in the breast reduction process.
Breast augmentation vs fat transfer explained honestly. Compare results, recovery, cost, candidacy, and mammogram impact to choose with confidence.

July 25, 2026
Considering split earlobe repair? Learn about causes, techniques, costs, healing, and how to choose a qualified surgeon for natural-looking results.

July 24, 2026
Explore laser skin rejuvenation in 2026, including ablative vs non-ablative options, recovery, risks, and how to choose a provider.
Cape Cod Plastic Surgery offers expert cosmetic and reconstructive procedures in a safe, accredited setting. Led by Dr. Marc Fater, we combine advanced techniques with personalized care to help you look and feel your best.
Monday: 9:00 AM – 5:00 PM
Tuesday: 9:00 AM – 5:00 PM
Wednesday: 9:00 AM – 5:00 PM
Thursday: 9:00 AM – 5:00 PM
Friday: 9:00 AM – 5:00 PM