
Breast Augmentation Before and After Pregnancy Guide
Compare breast augmentation before and after pregnancy with expert guidance on timing, breastfeeding safety, implant choices, and realistic results.
Jun 13, 2026

You've just had surgery. You're waking up, your mouth feels dry, the room is a little foggy, and when you try to focus on a face or a clock, your vision seems off. That can be unsettling fast.
Most of the time, blurry vision after anesthesia is temporary and not dangerous. It often comes from a dry eye surface, protective ointment, or medication effects rather than a serious injury to the eye. Still, there's an important distinction between normal post-op haze and symptoms that need urgent attention.
As a surgeon, I want patients to have both reassurance and a clear plan. If your vision is mildly blurry but steadily improving, that's usually comforting. If it's sudden, one-sided, painful, or not improving, that deserves a prompt call. The goal is not to panic. The goal is to know what's ordinary, what isn't, and what to do next.
One of the most common questions after surgery is simple: “Why is my vision blurry when nobody operated on my eyes?”
That question makes sense. People expect grogginess, soreness, and maybe nausea. They don't expect to look around the recovery room and feel as if someone has smeared a thin film across their glasses. For many patients, that moment is more alarming than painful.
The first thing I tell patients is this: blurry vision right after anesthesia is a known post-op symptom. In many cases, it reflects temporary changes on the eye's surface or short-lived effects from medications used during surgery and recovery. It doesn't automatically mean anything went wrong.
Practical rule: Mild blur in both eyes, especially when you're drowsy and dry, is often a recovery issue. Sudden major vision change is different.
Confusion usually comes from the word “blurry.” Patients use it to describe several different feelings:
Those details matter. They help us tell the difference between a common nuisance and something that needs urgent evaluation.
A helpful way to think about it is this. Your eyes are like camera lenses with a very delicate front surface. Surgery can temporarily disturb the “lens coating” even when the lens itself is fine. Typically, that clears as the body wakes up, the eyes rehydrate, and medications wear off.
The reassuring news is that the most frequent causes are usually minor and self-limited. They tend to fall into two buckets: surface irritation and medication-related focusing changes.
The cornea is the clear front window of the eye. I often compare it to a car windshield. If the windshield is clean and wet, you see clearly. If it's dry, dusty, or lightly scratched, everything looks smeared even though the rest of the car is working fine.
Under anesthesia, you don't blink normally. Your eyelids may not close as tightly as they do during natural sleep. That can dry the corneal surface unless it's protected carefully. Corneal exposure injury is the most common direct ocular cause of blurred vision after general anesthesia, and a cited review notes painful corneal abrasions occurred in about 1 in 2,800 patients after general anesthesia, with a broader ocular-complication rate of 2.3 cases per 10,000 anesthetics in that report's discussion of perioperative eye injury as summarized here.
What does that feel like in real life?
Most of these surface problems improve as the eye rehydrates and heals.
Some medications used around surgery affect the way the eye focuses. Instead of injuring the eye, they temporarily alter the muscles or nerve signals that help you shift focus, especially for reading or close-up work.
A common example is scopolamine, which is sometimes used to prevent nausea. Patients may notice dry mouth and hazy or blurry vision, especially up close. That kind of blur often behaves differently from a corneal problem. It may not hurt much, but your focusing feels “off.”
If your eyes feel dry, sandy, or sensitive to light, think surface irritation first. If they don't hurt but you can't focus well up close, a medication effect is often more likely.
Many people hear “dry eye” and assume that means only mild discomfort. But dry or irritated corneas can make vision surprisingly blurry. Others hear “anesthesia blur” and assume it's one single problem. It isn't. It's a symptom with several common explanations, and most of them are benign.
A final point that often gets overlooked is simple fluid shift. After surgery, your body may hold onto fluid temporarily, and that can subtly affect how crisp your vision feels. Patients often describe this as puffiness, heaviness, or a generalized haze rather than sharp eye pain.
Not all anesthesia works the same way, and that's one reason patients have different visual symptoms after surgery. A brief procedure with IV sedation doesn't create the same recovery pattern as a longer operation under general anesthesia, even if the symptom sounds similar.
With general anesthesia, you're fully unconscious. Your body relaxes, including the normal protective reflexes that help shield the eyes. You don't blink, you don't spread tears over the eye surface normally, and your care team has to protect the eyes for you during the procedure.
That's why eye protection during surgery matters so much. The blur afterward may come from dryness, protective ointment, or less commonly a superficial corneal injury. In other words, the issue is often mechanical and surface-related, not a sign that anesthesia “damaged” your eyesight.
For patients who want a plain-language overview of how sedation and anesthesia levels differ in another healthcare setting, this guide on sedation dentistry explained is a helpful comparison.
With twilight sedation or monitored anesthesia care, you may breathe on your own and recover faster, but medications can still leave you groggy and visually “slow.” People sometimes describe this as not quite blurry and not quite double, but hard to focus.
This matters in aesthetic surgery, where some procedures may use lighter anesthesia plans depending on the case. If you're comparing options, our overview of anesthesia types used for surgery explains the differences in a patient-friendly way.
One medication deserves its own mention because it confuses patients so often. Scopolamine, often given for nausea prevention, can cause hazy or blurred vision that usually improves within hours to about 24 hours after patch removal based on this patient-facing anesthesia discussion.
That timeline matters. If your blur clearly started around the time a scopolamine patch was used and then begins easing after removal, that pattern is reassuring. If it lingers well beyond that window, or comes with pain, marked asymmetry, or major visual loss, it needs a different explanation.
Patients usually want two answers: what's normal today, and when should I worry if it isn't gone yet?
The answer depends on the cause. Some blur clears quickly. Some takes a few days. A smaller group of patients notices that surgery seems to “bring out” a focusing problem they already had but didn't notice much before.
Here's the practical pattern I discuss with patients:
| Cause | What it often feels like | Typical course |
|---|---|---|
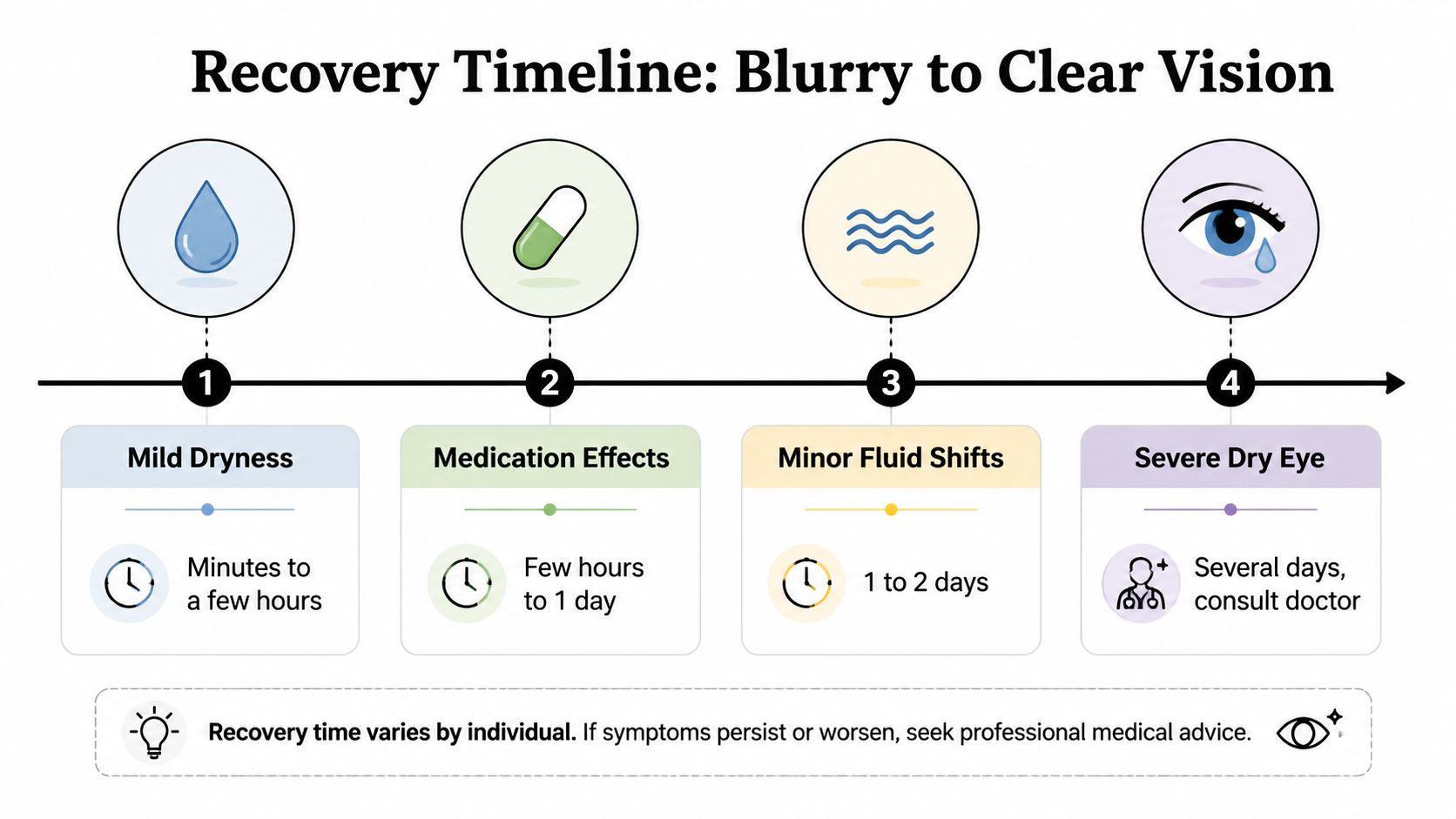
| Surface dryness or lubricant | Filmy, smeared, fluctuating vision | Often improves over hours or by the next day |
| Medication-related focusing change | Trouble reading, hazy near vision, dry mouth | Often fades as the medication wears off |
| Mild fluid-related haze | General fogginess, puffy feeling | Usually settles gradually |
| Refractive change becoming noticeable | Vision stays off even after you feel otherwise recovered | May persist longer and need an eye exam |
The most important principle is direction. If vision is improving, even slowly, that's reassuring. If it's worsening or staying distinctly abnormal, that changes the conversation.
A useful finding comes from a retrospective study summarized in postoperative anesthesia literature. New-onset blurred vision lasting at least 3 days occurred in 4.2% of 671 patients after non-ocular surgery, and 25% of those patients needed a new corrective lens or a change to an existing prescription within 18 months according to this review discussing that study.
That's important because not all lingering blur means injury. Sometimes surgery stress temporarily weakens focusing, and a preexisting need for glasses becomes more obvious. Patients often say, “I thought anesthesia caused this,” when what occurred is that recovery made an underlying refractive issue impossible to ignore.
A helpful way to think about this is that surgery can shake a loose tooth. It didn't create the tooth. It revealed the problem.
If your blur is mild and improving, the right next step is usually observation plus basic post-op care. If you're in the normal recovery phase after a cosmetic procedure, our patient guide to recovering from plastic surgery may help you keep the broader picture in view.
Contact your surgeon or anesthesia team sooner if:
This is the part I want every patient to remember. Most post-op blur is not dangerous. A small number of cases are urgent, and the safest approach is to know the difference.
I use a simple stoplight framework.
These are usually watch-and-wait symptoms if they're mild and steadily improving:
These deserve a call to your surgeon's office the same day:
Here's a quick patient education video that reinforces the idea that certain eye symptoms should never be ignored:
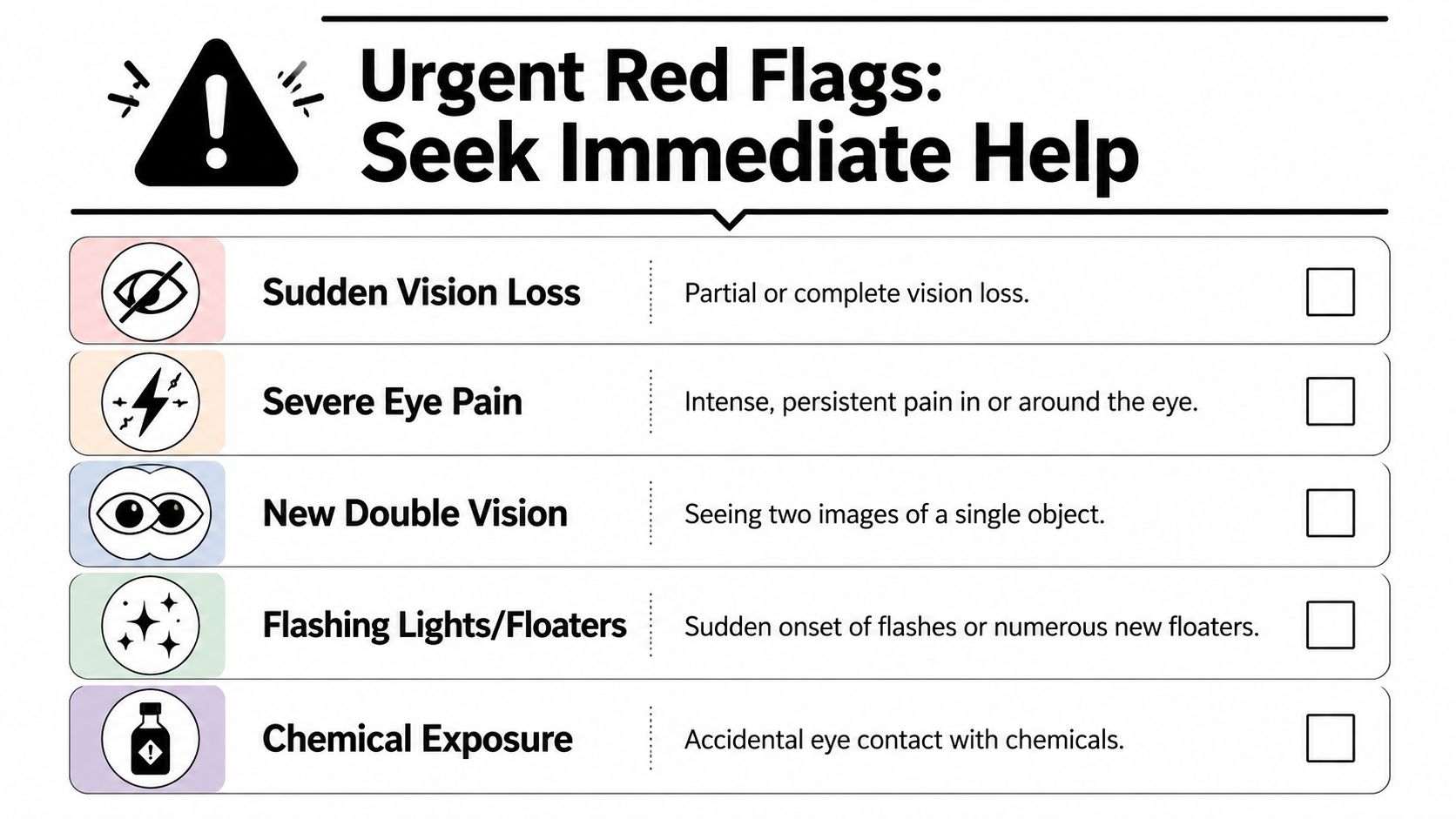
These require immediate medical attention, not routine follow-up:
For a practical public-facing checklist, this page on urgent eye care information is a useful reference.
Severe postoperative vision loss after non-eye surgery is very uncommon, with historical incidence estimates ranging from 0.056% to 1.3% overall, with higher-risk procedures including cardiac surgery at about 0.09% and spinal surgery as high as 0.2%. In the ASA Perioperative Visual Loss Registry collected from 1999 to 2012, 94% of ischemic optic neuropathy cases followed surgeries under general anesthesia lasting 6 hours or longer as reviewed in Frontiers in Surgery.
That risk profile matters because it helps frame context. The rare, severe causes are far more associated with long, complex operations than with routine outpatient cosmetic surgery. But “rare” doesn't mean “ignore it.”
Sudden, one-sided, or dramatic vision change is not something to monitor overnight at home.
If you're already familiar with the importance of watching for serious post-op complications in general, the same mindset applies here. Our education on preventing blood clots after surgery reflects the same principle: uncommon complications still deserve prompt action when warning signs appear.
Patients feel calmer when they know what their surgical team is doing before they ever wake up in recovery. Good post-op reassurance starts with good intraoperative protection.
We start with the history. If a patient already has dry eye symptoms, wears contacts often, has sensitive eyes, or has had prior eye procedures, that matters. It helps shape how we counsel them and how closely we watch for surface irritation afterward.
We also talk through nausea-prevention planning, because some anti-nausea medications can affect vision temporarily. Patients do better when they know in advance that a medication can cause hazy near vision for a short time.
Eye protection during surgery is deliberate, not casual. The eyes are kept closed and protected so the corneal surface doesn't dry out unnecessarily. That sounds like a small detail, but in anesthesia care, small details prevent big discomfort.
In an accredited surgical setting, that means consistent protocols rather than guesswork. Cape Cod Plastic Surgery performs procedures in an on-site AAAASF-accredited surgical suite, where patient eye protection is part of routine operative safety rather than an afterthought.
Clear instructions matter just as much as technical care. Patients need to know what level of blur is common, what symptoms suggest dryness or medication effect, and exactly when to call. That lowers anxiety and shortens the time between a real concern and proper evaluation.
I also encourage patients to describe the symptom precisely. “Blurry” is a start, but “my right eye feels scratched and light-sensitive” is more useful. “Both eyes are hazy but getting better” tells a different story than “I suddenly can't see well out of one eye.”
The best safety tool after surgery is often a simple, accurate symptom description given early.
Yes, it can be. The symptom is usually related to dryness, surface irritation, ointment, or medication effects rather than the specific cosmetic procedure itself. What matters most is how the symptom behaves. Mild and improving is usually reassuring. Sudden, one-sided, or persistent is not.
It can make recovery feel more confusing. A patient may have a mild preexisting refractive issue that becomes more noticeable after surgery and anesthesia. Patient-facing education on this topic often notes that about 1 in 25 patients may have blur lasting at least 3 days, and about 1 in 100 may still have fuzzy vision that doesn't resolve quickly and may need glasses or contacts, with the key point being that sudden, one-sided, or persistent change needs prompt evaluation as explained in this All About Vision overview.
Routine facial cosmetic surgery should not directly damage your vision in the usual course of recovery, but swelling, ointment, dryness, and post-op medications can make vision feel off temporarily. If the issue is only mild haze and it improves, that fits a common pattern. If you notice a major change in visual function, don't assume it's just swelling.
Be concrete. These details help:
When it started
Was it immediate in recovery, later that night, or the next day?
Whether it's one eye or both
One-sided symptoms raise more concern.
What it feels like
Hazy, scratched, painful, dim, doubled, or like a curtain.
Whether it's improving
Better, unchanged, or worse is one of the most useful clues.
Sometimes yes, sometimes no. If it's mild, symmetric, and clearly improving, observation may be reasonable. If it's sudden, severe, painful, or associated with loss of part of your vision, you should seek urgent help right away.
Not until your vision is clear enough and you're fully recovered from sedation or anesthesia. Even mild blur combined with residual grogginess can make driving unsafe. Arrange help in advance, and don't treat “almost clear” as good enough.
Most blurry vision after anesthesia is temporary. The mistake is assuming that all of it is harmless. If the change is sudden, one-sided, painful, or persistent, it needs prompt evaluation.
If you're preparing for surgery or have questions about recovery after a procedure, Cape Cod Plastic Surgery offers patient education, pre-op planning, and post-op guidance designed to help you recognize what's routine and when to reach out. If a visual symptom after surgery worries you, contact your surgical team promptly so they can guide your next step.
Compare breast augmentation before and after pregnancy with expert guidance on timing, breastfeeding safety, implant choices, and realistic results.

July 27, 2026
Learn evidence-based capsular contracture prevention strategies, from surgical technique and implant choice to aftercare and early warning signs.
July 26, 2026
Breast augmentation vs fat transfer explained honestly. Compare results, recovery, cost, candidacy, and mammogram impact to choose with confidence.
Cape Cod Plastic Surgery offers expert cosmetic and reconstructive procedures in a safe, accredited setting. Led by Dr. Marc Fater, we combine advanced techniques with personalized care to help you look and feel your best.
Monday: 9:00 AM – 5:00 PM
Tuesday: 9:00 AM – 5:00 PM
Wednesday: 9:00 AM – 5:00 PM
Thursday: 9:00 AM – 5:00 PM
Friday: 9:00 AM – 5:00 PM