
Fat Transfer vs. Filler: Your Ultimate 2026 Guide
Fat Transfer vs Filler: Our expert 2026 guide compares longevity, cost, recovery, and safety to help you choose your best option.
Jul 6, 2026

You see it in a familiar way. The cheeks look flatter in certain light. The temples seem a little hollow. Under the eyes, concealer starts doing more work than it used to. Most patients who ask about facial rejuvenation are not trying to look different. They're trying to look less tired, less drawn, and more like themselves.
That's where the fat transfer vs filler decision usually begins.
Both treatments restore volume. Both can soften the signs of facial aging. But they are not interchangeable. One uses your own living tissue. The other uses an injectable product designed to add shape and support. One is a minor surgical procedure with recovery. The other is usually an office treatment with immediate visible change.
Those differences matter more than most online comparisons suggest. Longevity matters. Downtime matters. Cost matters. But the deeper distinction is biological. Fat can integrate, soften, and behave like part of your face because it is part of your biology. Fillers are excellent tools, but they remain implanted material that adds volume and then gradually breaks down.
Patients do best when they understand the trade-offs before choosing. A sharper jawline for an event next month is a different goal from rebuilding cheeks or temples in a durable, natural-feeling way. Under-eye correction is its own category entirely.
A common consultation starts with a patient saying, “I'm not sure what changed, but my face looks tired.” Usually, the issue isn't just skin laxity or lines. It's volume loss.
When facial fat shifts and diminishes, the face can look less supported. Cheeks flatten. Temples hollow. The area under the eyes can start to cast shadows. At that point, most patients are deciding between the two main tools available today: fat transfer and dermal fillers.
The choice sounds simple on the surface. Do you want to use your own tissue, or a ready-made injectable product? In practice, it's more nuanced.
Some patients want a quick, adjustable treatment with almost no interruption to daily life. Others want a more lasting change and are willing to accept a procedure and recovery to get there. Some need broad, soft restoration across multiple areas. Others need precise refinement in a very small zone.
The best treatment isn't the one that sounds most advanced. It's the one that matches your anatomy, your tolerance for downtime, and the way you want your result to age over time.
That's why fat transfer vs filler shouldn't be framed as a winner-and-loser debate. They solve different problems well. In some patients, they can even complement each other. But if you understand the biological differences from the start, the decision gets much clearer.
The mechanics of these treatments are very different. That difference affects planning, recovery, and the type of result you can expect.
Fat transfer is a two-part surgical procedure. First, fat is harvested through liposuction from an area such as the abdomen or thighs. Then that fat is processed so the healthiest cells can be placed back into the face with careful, layered injections.
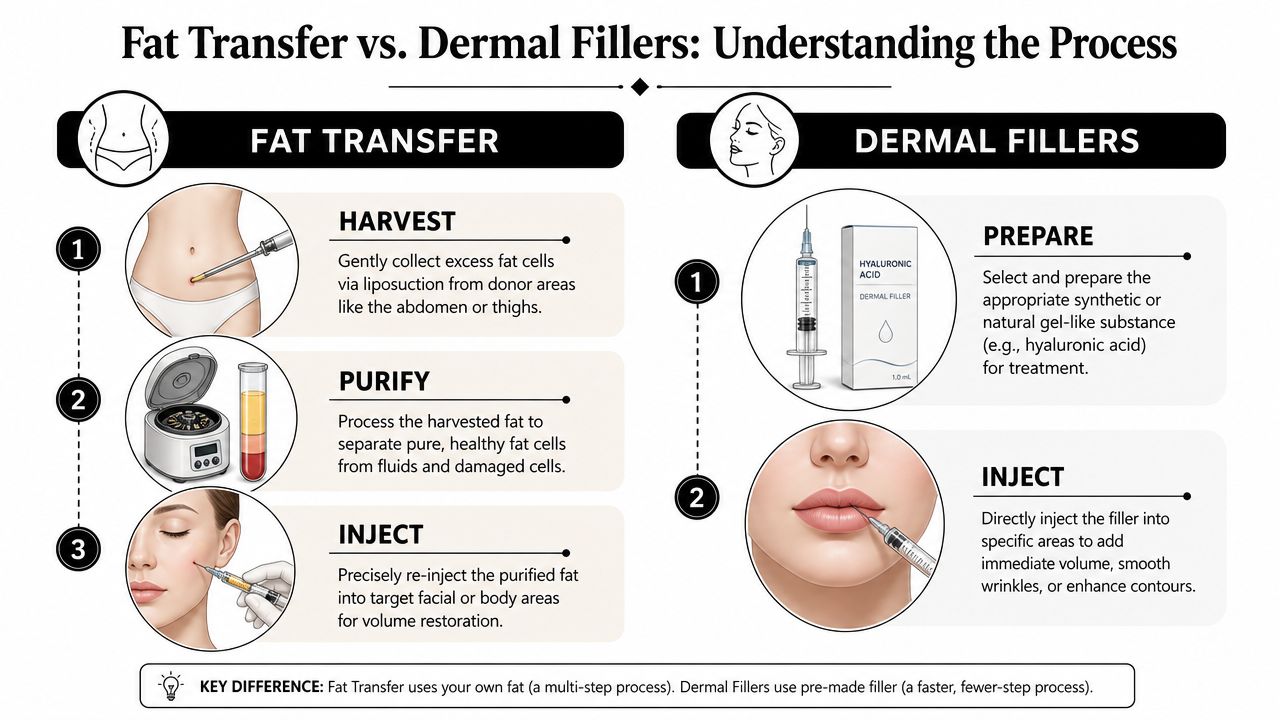
That matters because the surgeon does more than “fill” a space. Fat transfer is a transplant of living cells. Those cells need to establish a blood supply in their new location. Some survive and integrate. Some do not.
The basic flow looks like this:
Fat transfer is also more involved from a patient experience standpoint. It's a dual surgical procedure involving harvesting and grafting, and it typically requires approximately 7 to 10 days of social downtime, while fillers are non-surgical office visits with minimal downtime and immediate results, as described in this plastic surgeon's guide to fat grafting vs fillers.
Dermal fillers are more straightforward. A prepackaged gel, commonly a hyaluronic acid filler, is injected directly into a target area to restore volume, smooth transitions, or refine contours. There's no donor site, no harvesting, and no graft processing.
For many patients, that simplicity is the appeal. The appointment is usually shorter, the result is visible right away, and recovery is much easier to fit into a normal schedule. If you want a more detailed overview of products and treatment planning, this guide on dermal fillers explained is a useful companion.
With filler, the product provides volume the moment it's placed. With fat transfer, volume develops through survival and integration of living cells. That's why fat transfer demands more patience and more surgical judgment.
One treatment relocates your own tissue. The other places a manufactured gel into a carefully selected space. That single distinction drives nearly every trade-off that follows.
The most important difference in fat transfer vs filler is not just how long each lasts. It's what the material is.
Fat is living tissue. Filler is a gel. That's the starting point for understanding why the results feel, settle, and age differently.
Transferred fat cells carry regenerative potential. The verified clinical background provided for this article notes that fat releases growth factors that stimulate natural collagen and elastin synthesis and support new blood vessel formation, while fillers add passive volume and degrade over time without improving the biological quality of surrounding tissue.
That doesn't mean filler is inferior. It means filler is doing a different job. It is an excellent structural tool when you want a controlled amount of lift, contour, or smoothing in a defined area. Fat transfer is often more appealing when the goal is broad restoration with a softer, more integrated feel.
Many patients need the clearest explanation at this point.
Fillers are highly predictable in volume because what is injected is what is providing the visible correction. Fat transfer is more variable because not every transferred cell survives. Scientific literature reports a broad survival range of 20% to 90%, with numerous studies showing a typical retention rate of 50% to 70% after the early postoperative period, as discussed in this review of fat grafting versus dermal fillers for long-term results.
That means filler is usually better when a patient wants exact, measured correction in a small space. Fat transfer is often better when a patient wants a biologic, softer-volume restoration and accepts some variability in how much survives.
| Characteristic | Fat Transfer | Dermal Fillers |
|---|---|---|
| Source material | Your own fat cells | Injectable gel, commonly hyaluronic acid |
| Procedure type | Minor surgical procedure with harvest and grafting | Non-surgical office injection |
| Result timing | Develops as grafted fat settles and survives | Immediate visible volume |
| Volume predictability | Less predictable because cell survival varies | More predictable at the time of injection |
| Tissue behavior | Integrates as living tissue | Adds structural volume, then gradually degrades |
| Skin-quality effect | May offer regenerative benefit through growth factors and stromal activity | Primarily volumizing, not regenerative |
| Best fit | Broad facial restoration, soft contour, larger-volume needs | Fine-tuning, precise shaping, temporary enhancement |
Patients often focus first on mirrors and photos. Surgeons also think about how a correction behaves over time. Fat that survives becomes part of the area. It tends to move and blend more like native tissue. Fillers can look excellent, especially in skilled hands, but they remain placed product.
Clinical takeaway: If the goal is exact adjustment, filler usually has the edge. If the goal is integrated facial volume using your own tissue, fat transfer often has advantages that go beyond longevity.
Patients usually narrow this decision around three questions. How long will it last? How much downtime is involved? What does the investment look like over time?
Fat transfer asks for patience on the front end. The long-term viability of fat transfer is defined by a fat survival rate of approximately 50%, but once stabilized, the result is considered permanent. By contrast, dermal fillers typically last 6 to 24 months, making fat grafting potentially more cost-effective over a multi-year horizon, according to this discussion of how fat transfer compares with fillers over time.
That permanence is appealing to patients who don't want repeated maintenance appointments. It's less appealing to someone who wants a reversible first step.
The recovery experience is not subtle. Fillers fit more easily into a normal week. Fat transfer usually does not.
With fillers, most patients return to regular activities quickly. With fat transfer, there are two treatment areas to consider: the donor site where fat was harvested, and the face where fat was placed. Swelling and bruising can make patients look socially off-duty for a period of time even when healing is progressing normally.
For many people, that's the deciding factor.
A single filler visit usually feels more approachable because the upfront expense is lower. Fat transfer usually carries a higher initial cost because it is a procedure, not just an injection appointment.
But cost has to be measured across time, not just at checkout. If a patient wants ongoing correction with filler, that usually means maintenance. If a patient wants a more lasting volume restoration and is a good candidate for fat transfer, the larger upfront investment can make more sense over several years. For patients still comparing timelines, this overview of how long filler lasts can help frame the maintenance side of the decision.
The right treatment often becomes obvious once you match it to the area being treated.

Fat transfer tends to perform best when the problem is not a single crease, but a broader pattern of deflation. Hollow temples, flat cheeks, and diffuse facial volume loss often respond well because fat can restore a softer, more continuous contour.
It is also useful when larger-volume correction would otherwise require repeated filler treatments over time. In those cases, using the patient's own tissue can create a result that feels more integrated and less “injected.”
Common examples include:
Fillers excel in areas that demand precision and immediate control. Lips are a classic example. So are fine contour adjustments along the jawline, or carefully selected corrections in folds and transitions where tiny volume changes matter.
That doesn't mean filler is only for small treatments. It means the strength of filler is precision.
A surgeon often reaches for filler when the treatment plan calls for exact shaping. A surgeon often prefers fat when the treatment plan calls for restoration.
Patients considering the under-eye area should also review a focused explanation of tear trough treatment options, because that region behaves differently from the cheeks or jawline.
The tear trough is where simplistic fat transfer vs filler advice often breaks down. This is delicate, thin-skinned anatomy. A treatment that looks good in the syringe doesn't always look good through the skin.
A critical but often overlooked factor is the Tyndall effect. Clinical data from periorbital surgery indicates that fat grafting integrates naturally and avoids the bluish discoloration that can occur with superficially placed hyaluronic acid filler in the tear trough, as noted in this clinical discussion of periorbital fat grafting.
For the right patient, that's a major advantage. Under-eye rejuvenation isn't just about filling a hollow. It's about preserving natural color, texture, and transition from lower eyelid to cheek.
For a visual explanation of how surgeons think about these options in practice, this overview is helpful:
A treatment can be effective and still be wrong for a specific patient. Safety always comes first.
Autologous fat transfer has a strong safety profile in facial rejuvenation when performed appropriately. A systematic review reported an overall complication rate of 6%, with the most common issues being hematoma or ecchymosis at 5%, fat necrosis at 2%, and irregular fat distribution at 2%. The same review found a complete absence of hypersensitivity reactions and granuloma formation, and major complications associated with hyaluronic acid fillers, such as tissue necrosis and blindness, were not reported in the reviewed fat transfer cases, according to this systematic review of autologous fat transfer safety.
That absence of allergic or hypersensitivity risk makes sense biologically. The graft comes from your own body.
Fat transfer carries procedural risks related to harvesting and graft placement. These include bruising, swelling, contour irregularity, and the possibility that some fat won't survive as intended. Fillers avoid the donor-site aspect but bring their own set of issues, including malposition, visible irregularity, and vascular complications in rare but serious cases.
The practical point is simple. A patient should not choose a treatment because it sounds easier or more natural. A patient should choose it because the risks of that treatment fit the anatomy and the goal.
The ideal candidate for each option usually looks different.
Not every hollow area needs surgery. Not every volume loss problem should be managed with repeated syringes. Good planning matters more than loyalty to one technique.
Most patients don't need more opinions from social media. They need a clear framework.
Start with a few honest questions. Do you want something temporary or something intended to last? Are you comfortable with a minor surgical procedure and a recovery period? Is your priority exact short-term control, or a softer long-term restoration using your own tissue?
If you want immediate change, low downtime, and flexibility, fillers often make sense. If you want a more durable result and you're willing to go through harvesting, healing, and the variability that comes with living tissue transfer, fat transfer may be the better fit.
That decision also depends on where the treatment is being done. A small lip enhancement is a very different problem from restoring a hollow temple or rebuilding facial volume after age-related deflation. Under-eye correction, in particular, deserves careful judgment because the wrong material in the wrong plane can look obvious.
No article can assess your facial structure, skin thickness, donor-fat availability, or how your features balance in motion. That's the work of an in-person consultation with a board-certified plastic surgeon who performs facial volume restoration regularly and can explain not just what can be done, but what should be done.
A good consultation should leave you with more than a quote. It should answer:
If you're comparing fat transfer vs filler seriously, the next step shouldn't be guessing. It should be a personalized evaluation with a qualified expert who can align the plan with your anatomy and your goals.
Fat transfer requires fat harvesting, so there are small access points where liposuction is performed. In well-planned cases, these are typically placed as discreetly as possible. Most patients are far more aware of swelling and bruising early on than the harvest marks themselves.
Yes. In selected patients, combining them can make sense. Fat transfer can rebuild broader foundational volume, while filler can refine a smaller area that benefits from precise shaping. The key is not stacking treatments casually. The plan has to be coordinated so one treatment doesn't compromise the aesthetic logic of the other.
The verified clinical background for this article notes that long-term fat graft volume is influenced primarily by patient weight fluctuations. Once the surviving cells establish a blood supply, they become a living part of your tissue and can expand or contract naturally with weight changes.
There isn't one correct age. Candidacy depends more on anatomy, goals, medical history, and whether the issue is true volume loss or something else. Younger patients often seek contouring or under-eye correction. Older patients may be addressing broader facial deflation. Age matters less than choosing the right treatment for the right reason.
Either can look natural when properly selected and well performed. Problems arise when the wrong material is used in the wrong area, or when too much product is placed. In general, fat often has an advantage when the goal is broad, soft restoration. Fillers often have an advantage when the goal is precise control.
Not automatically. Less invasive doesn't always mean lower-stakes. Fillers avoid a donor procedure, but they still require deep anatomical knowledge and careful technique. Fat transfer is more involved, yet it has the benefit of using your own tissue and avoids hypersensitivity concerns. Safety depends on the treatment, the anatomy, and the person performing it.
If you're weighing these options and want a personalized recommendation, schedule a consultation with Cape Cod Plastic Surgery. Dr. Marc Fater is a board-certified plastic surgeon in Hyannis who can evaluate your facial anatomy, explain whether fat transfer, filler, or a combination makes the most sense, and build a plan focused on safe, natural-looking results.
Fat Transfer vs Filler: Our expert 2026 guide compares longevity, cost, recovery, and safety to help you choose your best option.

July 6, 2026
Your Journey to a Renewed Silhouette: Recovering from Post-Weight-Loss Surgery

July 5, 2026
Tired of frown lines? Learn how to get rid of wrinkles between eyebrows with at-home tips, Botox, fillers, and more from a board-certified plastic surgeon.
Cape Cod Plastic Surgery offers expert cosmetic and reconstructive procedures in a safe, accredited setting. Led by Dr. Marc Fater, we combine advanced techniques with personalized care to help you look and feel your best.
Monday: 9:00 AM – 5:00 PM
Tuesday: 9:00 AM – 5:00 PM
Wednesday: 9:00 AM – 5:00 PM
Thursday: 9:00 AM – 5:00 PM
Friday: 9:00 AM – 5:00 PM