
Your Guide to Tear Trough Treatment in Cape Cod
Considering tear trough treatment? This guide explains fillers, fat transfer, and surgery options at Cape Cod Plastic Surgery to refresh your look.
Jul 1, 2026

You wake up feeling fine, sleep was decent, and your energy is there. Then you catch your reflection in the bathroom mirror and see the same thing you saw yesterday: shadows under the eyes, a hollow groove, maybe a little puffiness, and an expression that looks more exhausted than you feel.
That disconnect frustrates a lot of people. Friends may say you look tired. You may try concealer, better skincare, more water, more sleep, and still feel like the under-eye area gives you away.
The reason is often anatomical, not lifestyle-related. In many patients, the issue is a tear trough, the natural groove that starts near the inner corner of the eye and continues down toward the cheek. When that groove becomes more visible, it creates a valley-like shadow. On the face, shadows often read as fatigue, even when the skin itself is healthy and the person feels well.
A tear trough isn't a disease or a flaw. It's part of normal facial structure. Some people have it because of genetics and notice it young. Others see it deepen over time as the tissues around the eyes change and the transition between the lower eyelid and cheek becomes less smooth.
Think of the lower eyelid and upper cheek as a continuous surface. When the surface is even, light reflects smoothly. When a groove forms, light falls into that depression and creates a darkened shadow. That's why many people say, “I look like I have dark circles,” when the true issue is hollowness, not pigment.
That distinction matters because different under-eye problems need different treatments. A hollow groove is not the same thing as loose skin. It isn't the same thing as fat bulging forward. And it definitely isn't the same thing as skin discoloration.
A good under-eye consultation starts with one question: is the problem a shadow from volume loss, or is it something else entirely?
People often come in asking for “tear trough filler” when what they really want is a fresher, more rested appearance. Those aren't always the same thing. Sometimes filler is the right answer. Sometimes fat transfer makes more sense. Sometimes lower eyelid surgery is the treatment that corrects the anatomy. And sometimes the under-eye area shouldn't be filled at all.
Understanding that difference is what protects patients from disappointing results and unnecessary risk.
The most important part of tear trough treatment isn't the syringe or the surgery. It's the diagnosis.
A common mistake is assuming that every under-eye concern is caused by volume loss. It isn't. Some people have a true hollow. Others have under-eye puffiness, protruding fat pads, or festoons. If you place filler into an area that already looks full or swollen, you can make it look heavier.
A key warning from a referenced discussion of this issue is that pre-existing under-eye puffiness or fat pads are a critical contraindication for tear trough filler, and retrospective studies have shown that 30% of dissatisfaction cases in tear trough augmentation stem from misdiagnosis of the underlying cause (discussion of diagnosis-first under-eye assessment).
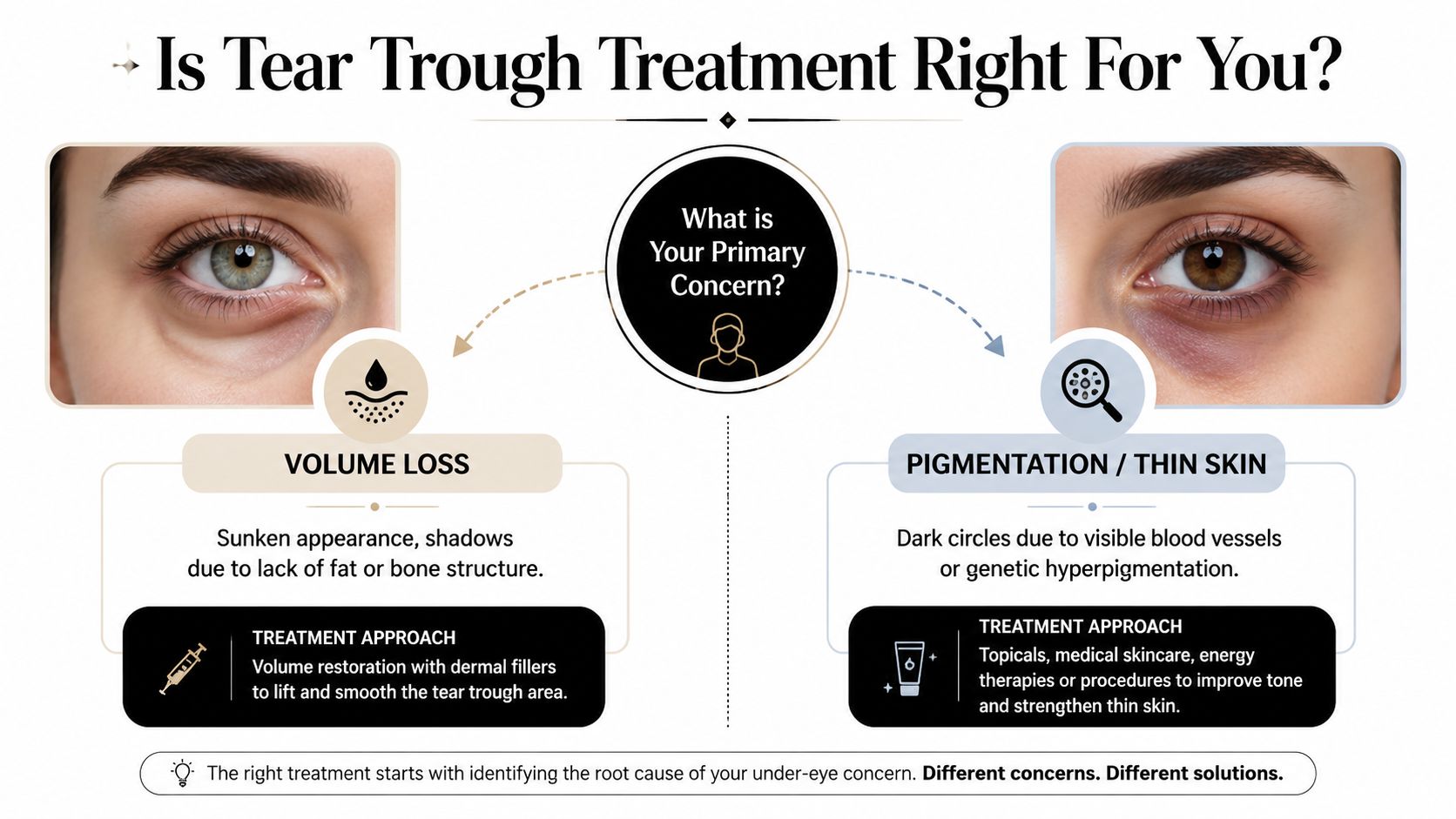
If you have a true tear trough deformity, the under-eye area tends to look sunken. The groove is more visible in certain lighting. Makeup may settle there. The problem often looks like a shadow or indentation.
If the issue is puffiness, the lower eyelid looks raised, swollen, or baggy. In that case, the area doesn't need more volume. It usually needs a different strategy.
Here is a simple way to view it:
Patients who do well with nonsurgical tear trough treatment often share a few features:
If your concern sounds more like a hollow than a bag, a detailed evaluation is the next step. For a helpful patient-friendly overview of under-eye hollows, see this article on how to get rid of under-eye hollows.
Practical rule: If the lower eyelid already looks full in profile, filler may not be the treatment you want, even if the area also looks dark.
A patient might say, “I have dark circles.” That phrase can describe several different problems:
Many online guides, however, oversimplify the issue. They treat “dark circles” as one diagnosis. In practice, it's a category, not a conclusion.
If a surgeon or injector doesn't separate hollowness from puffiness, the wrong treatment can look unnatural. A careful in-person exam is what determines whether you need volume restoration, surgical contouring, skin-focused care, or a combination.
For the right patient, hyaluronic acid dermal filler can be an elegant way to soften a tear trough. Hyaluronic acid is a substance naturally found in the body. In the under-eye area, its job is simple: it restores subtle support where a groove has formed.
The easiest way to picture it is a cushion that has flattened slightly over time. The goal isn't to overstuff it. The goal is to gently re-inflate it so the transition from eyelid to cheek looks smoother.

This is one of the most delicate places on the face to inject. Technique matters as much as product choice.
A published approach to tear trough correction describes precise supraperiosteal injection at 0.5 to 0.7 mL per eye using a 25 to 27 G blunt cannula with a fan technique and 20 mg/mL HA filler (VYC-20L), specifically to help avoid vessel injury and the Tyndall effect. That same reference notes this approach is suitable for Stage 1A, which is insufficient volume without ptosis, and not for Stage 1B, where volume loss is combined with ptosis and filler can worsen descent (technical guidance on tear trough injection technique).
A blunt cannula is often preferred because it glides through tissue differently than a needle and can reduce trauma in this fragile area.
Most filler treatments are done in the office. The area is assessed carefully, marked, cleansed, and then treated with small, controlled amounts of product. Results are visible right away, although the under-eye region still needs time to settle.
Expert benchmarks note that patients often see correction immediately, with 1 to 2 weeks of settling time, and that low-viscosity HA is considered safe, while high-viscosity or nonbiodegradable products are contraindicated in this area because of nodule and vascular occlusion risk (expert benchmarks for tear trough filler longevity, cost, and product selection).
If you're trying to understand hyaluronic acid more broadly, including why it attracts water and is used across aesthetic medicine and skincare, this overview of how ingredients can achieve firmer smoother skin gives useful background.
For a broader patient guide to injectable options, this explainer on dermal fillers explained types results and safety is also worth reading.
In a prospective study of 24 patients, tear trough treatment with a cannula and a maximum of 1 mL of hyaluronic acid filler per session for both eyes showed 100% overall improvement in tear trough appearance, with 75% satisfaction after one session. The remaining 25% needed additional filler for full satisfaction. The study reported no major complications, only minor transient bruising and swelling resolving within 4 weeks, and noted that 4 out of 24 patients reported puffiness within the first 2 weeks, without correlation to filler volume. The authors also recommended 4-week follow-up as the minimum interval before adding more filler (prospective cannula study on tear trough filler safety and outcomes).
That study also noted an important practical point: patients over 35 years may need more than one session or more than 1 mL divided between both eyes.
Good tear trough filler should be hard to notice. People may think you look rested. They shouldn't think you look “done.”
Filler can soften a hollow. It doesn't remove skin. It doesn't reposition bulging fat. It doesn't treat every kind of dark circle.
That is why conservative treatment is best. In this area, more product isn't better. Better diagnosis, precise placement, and restraint are what create a natural result.
Later in the decision process, filler is often best viewed as the least invasive option for the right anatomy, not the universal answer for every under-eye complaint.
A brief visual overview can also help if you're deciding whether this treatment matches your goals.
Autologous fat transfer means using your own tissue to restore your own volume. Instead of placing a manufactured filler, the surgeon takes a small amount of fat from another part of the body, prepares it carefully, and then injects it into the hollow under-eye area.
For many patients, that idea feels intuitive. You're replacing missing volume with living tissue from your own body.
There are two main parts to fat transfer.
First, a small amount of fat is harvested from an area with available donor fat. Common donor sites include the abdomen or thighs. The amount removed is modest because the under-eye area requires precision, not bulk.
Second, the fat is processed and then placed in tiny amounts into the tear trough and nearby contour depressions. The goal is a smooth transition, not a puffy lower lid.
Fat transfer appeals to patients who want a more lasting solution and who are comfortable with a procedure that is more involved than filler.
A retrospective analysis of 155 patients treated with tear trough hyaluronic acid filler found that significant improvement persisted up to 18 months, challenging the older belief that results last only 6 to 12 months. The study reported a mean follow-up of 785 ± 536 days, with no significant differences in MIHAS grade changes between 6, 12, and 18 months, and patients evaluated at 18 months were less likely to show a change in MIHAS grade than those at 6 months (retrospective study on long-term tear trough HA filler durability).
That's impressive longevity for filler. Fat transfer, however, is chosen for a different reason. It aims for permanent integration of living fat cells rather than a temporary implantable gel.
Fat transfer often makes sense for someone who:
This option can be especially attractive when the tear trough is part of a broader facial volume loss pattern. In that setting, fat can restore softness in a way that feels very natural.
It is still technique-sensitive. The under-eye area remains unforgiving, and the treatment has to be planned with the same diagnostic care used for filler and surgery.
When the under-eye problem is bags, puffiness, loose skin, or a structural contour issue, lower blepharoplasty is often the most effective option. This is the operation designed to correct anatomy, not just camouflage it.
If filler is like softening a valley, surgery is about reshaping the natural contours.
Lower blepharoplasty can address concerns that filler can't solve well:
This is why patients with puffiness often do better with surgery than with filler. If the lower lid already projects outward, adding volume usually doesn't create a cleaner contour. Surgical correction can remove or reposition fat and refine the contour directly.

A patient with lower eyelid bags may spend time and money chasing less invasive treatments and still feel dissatisfied because the true issue was never corrected. Surgery changes that equation. It treats the source.
That doesn't mean every patient needs an operation. It means surgery is often the right treatment when the diagnosis points to puffiness, fat prolapse, or skin excess.
Surgery is not a failure of nonsurgical care. For the right anatomy, it is the most logical treatment.
A lower blepharoplasty is more involved than office-based filler. It requires healing time and careful postoperative care. In exchange, it can provide a more complete and longer-lasting improvement in the lower eyelid.
Patients usually value surgery when they want:
The best surgical outcomes are subtle. The lower eyelids should look smoother and less heavy, while still looking like your own eyes.
That is the central advantage of lower blepharoplasty. It is designed for the problem filler cannot fix well, which is fullness where there should be a clean lid-cheek junction.
A side by side comparison is helpful, but only after the diagnosis is right. Under-eye treatment is not like choosing between three versions of the same procedure. It is closer to choosing the right tool for a specific repair. If the problem is a hollow, one option may work well. If the problem is puffiness or festoons, that same option can make the area look heavier.
That is the mistake patients most often need help avoiding. A person may come in asking for filler because they look tired, but the under-eye area may be full rather than hollow. In that setting, adding volume does not correct the contour. It can worsen it.
| Factor | Dermal Fillers | Fat Transfer | Lower Blepharoplasty (Surgery) |
|---|---|---|---|
| Best candidate | A patient with a true tear trough hollow, good skin quality, and little to no puffiness | A patient with under-eye volume loss who prefers using their own tissue and accepts a more involved procedure | A patient with bags, fat prolapse, skin laxity, or a lid-cheek contour problem that needs structural correction |
| Procedure setting | Office-based injectable treatment | Procedure that includes fat harvesting and careful reinjection | Operating room or surgical setting |
| Recovery | Usually the shortest recovery. Swelling or unevenness can take time to settle | More recovery than filler because both the donor area and the under-eye area need to heal | The longest recovery of the three, but it addresses problems injectables cannot remove |
| How long results last | Temporary | Long-lasting volume restoration, though some fat survival varies by patient | Long-lasting structural improvement |
| Typical cost | Lower upfront cost, but maintenance may be needed | Higher than filler in many cases because it is a procedural treatment | Varies based on the surgical plan, facility, and technique |
| Main strength | Least invasive option for the right hollow | Uses your own tissue and can look very natural in selected patients | Best option when fullness, bags, or extra skin are part of the concern |
| Main limitation | Can look worse if puffiness, festoons, or malar edema are mistaken for hollowness | Healing is more involved, and graft take is not perfectly predictable | Requires surgery, healing time, and careful preoperative planning |
Recovery matters, but so does what you are recovering for. A shorter downtime is only an advantage if the treatment fits the anatomy. Many disappointing under-eye results happen because the least invasive option was chosen for the wrong reason.
Here is the practical way I explain it during a consultation:
Cost deserves an honest discussion too. Filler often looks less expensive at the start, but repeat treatments can add up over time. Surgery and fat transfer usually involve a larger initial investment, yet they may provide a more durable result for the right patient. The best value is not the lowest price. It is the treatment that solves the actual problem with the fewest revisions and the lowest chance of looking overtreated.
That is why surgeon judgment matters so much in this area. If you are comparing options locally, our guide to choosing among Cape Cod plastic surgeons can help you understand what to ask. For readers interested in the team behind the digital strategy supporting practices like this, you can also review Leaping Lemur Media's offerings.
There is no single best treatment for every tired-looking under-eye. There is a best match between anatomy and treatment plan. That is the difference between camouflage and correction.
Under-eye treatment is one of the clearest examples of why provider skill matters more than trend, product, or marketing. The anatomy is delicate, the skin is thin, and small differences in judgment can produce very different outcomes.
The technical literature makes that point directly. Expert tear trough treatment requires precise supraperiosteal injection using specific techniques and filler types to avoid vessel injury and the Tyndall effect, which is why experience matters so much in this area. That is also why patients should look for a surgeon or injector with deep familiarity with lower eyelid anatomy, not just general experience with facial fillers.
A thoughtful patient should ask whether the doctor can do three things well:
If you're researching credentials locally, this profile of Cape Cod plastic surgeons is a useful place to start.
A well-run practice also helps patients understand information clearly before they ever arrive for consultation. For clinics improving how they communicate educational content online, resources like Leaping Lemur Media's offerings can be helpful in thinking about patient education and digital experience.
The best under-eye result starts with hearing, “You are not a filler candidate,” when filler isn't right for you.
That kind of honesty is what protects both safety and aesthetics.
If you're considering Cape Cod Plastic Surgery, the next step is a one-on-one consultation focused on diagnosis first. Dr. Marc Fater and his team can evaluate whether your under-eye concern is true hollowness, puffiness, skin laxity, pigment, or a combination, then recommend the treatment that fits your anatomy and goals.
Considering tear trough treatment? This guide explains fillers, fat transfer, and surgery options at Cape Cod Plastic Surgery to refresh your look.

July 1, 2026
Transforming Your Body and Improving Wellness After Massive Weight Loss

June 30, 2026
Understand the full gynecomastia surgery cost in 2026. This guide breaks down fees, factors, insurance, and financing options to help you plan your budget.
Cape Cod Plastic Surgery offers expert cosmetic and reconstructive procedures in a safe, accredited setting. Led by Dr. Marc Fater, we combine advanced techniques with personalized care to help you look and feel your best.
Monday: 9:00 AM – 5:00 PM
Tuesday: 9:00 AM – 5:00 PM
Wednesday: 9:00 AM – 5:00 PM
Thursday: 9:00 AM – 5:00 PM
Friday: 9:00 AM – 5:00 PM